COMP/PSCP Vendors, Vehicles, and the Mandatory Floor That Lives in One Subaccount
T-5 East and T-5 West contract specifics, the $3.139 billion FY27 mandatory request that lands entirely in Base Operations and Communications, the BAP pause and what it means for TRICARE pharmacy, the operational record from GAO, DOT&E, the VA OIG, and the T-5 transition, the CDMRP “$1.5 billion cut” decoded, the HAC-D 119th Congress watchlist, and action windows tied to the June 11 subcommittee mark-up and the June 24 Full Committee mark-up.
★ Premium Capture Corner
The COMP/PSCP exposure map for incumbents and challengers, the full T-5 East/West contract picture, the BAP pause, the FY27 mandatory funding concentration, the CDMRP zero-out decoded, the operational record from GAO/DOT&E/VA OIG, the HAC-D 119th Congress watchlist, and action windows tied to June 11 and June 24. Free members see the headline; premium gets the full briefing.
See premium plansMMT Premium Exclusive: T-5 East and T-5 West contract specifics, the $3.139 billion FY27 mandatory request that lands entirely in Base Operations and Communications, the BAP pause and what it means for TRICARE pharmacy, the operational record from GAO, DOT&E, the VA OIG, and the T-5 transition that documents why the reattract goal could not have bent the line, the CDMRP “$1.5 billion cut” decoded, the HAC-D 119th Congress watchlist, and action windows tied to the June 11 subcommittee mark-up and the June 24 Full Committee mark-up.
Editor’s note on reporting limits. This issue ships Thursday, May 8, with the public reporting record that exists as of Wednesday evening, May 7. Two phone-call follow-ups were on the desk and were not made: (1) a call to Rep. Houlahan’s office on whether the cancelled March 25 hearing has a reschedule date, and (2) a call to the DHA Office of Small Business Programs on whether the Hicks 7 percent reattract goal is being treated as live policy, walked-back policy, or operationally inactive ahead of its December 31, 2026 expiration. Premium subscribers should know that ceiling. The rest of this issue is sourced from the J-Book, the Federal Advisory Committee Act database, the Houlahan-Fallon correspondence on file, the GAO May 5 dashboard, primary contract records (HigherGov, USASpending, GAO bid protest decisions), the May 6-7 BAP P&T Committee meeting record, GAO oversight reports on MHS GENESIS and VA EHRM, DOT&E operational test reports, peer-reviewed clinical research on MHS GENESIS usability, the VA OIG Oracle Cerner reports, NDAA report language directing DOD reporting on the T-5 transition, and provider association letters to Congress on the TRICARE crisis.
The public issue covered the analytical frame: the COMP and PSCP split is the budget structure catching up to the obligation behavior both DHA and VA have been operating at scale. This Capture Corner names the vendors, names the contract numbers, names the dollars, and names the subaccount where the FY27 mandatory layer actually lands.
Three things need to be clear before any positioning move.
First, the COMP and PSCP split is not a contract restructure. The TRICARE managed care support contracts, the MTF infrastructure programs, and the medical research and development activity are not changing form on October 1. What changes is which appropriation line they draw from and which subcommittee mark-up the funding flows through.
Second, the FY27 $3.139 billion COMP mandatory request lands in one subaccount. Not spread across COMP. One subaccount: Base Operations and Communications. Every other COMP line sits at $0 mandatory: In-House Care, Consolidated Health Support, Information Management, Management Activities, Education and Training, RDT&E, Procurement. The FY26 reconciliation precedent (P.L. 119-21) was $1.687 billion split across three subaccounts. The FY27 request escalates Base Ops alone by 3.5 times the FY26 Base Ops mandatory and asks for it as recurring mandatory authority rather than a one-time emergency layer.
Third, the policy commitment that was supposed to make COMP grow share against PSCP, the December 31, 2026 reattract goal, has not been hit, has not been formally walked back, and has not been replaced. Capture timing for FY28 budget moves runs through whatever the Department says or does not say about that goal between now and the next budget submission.
Here is the playbook.
The picture, on one chart
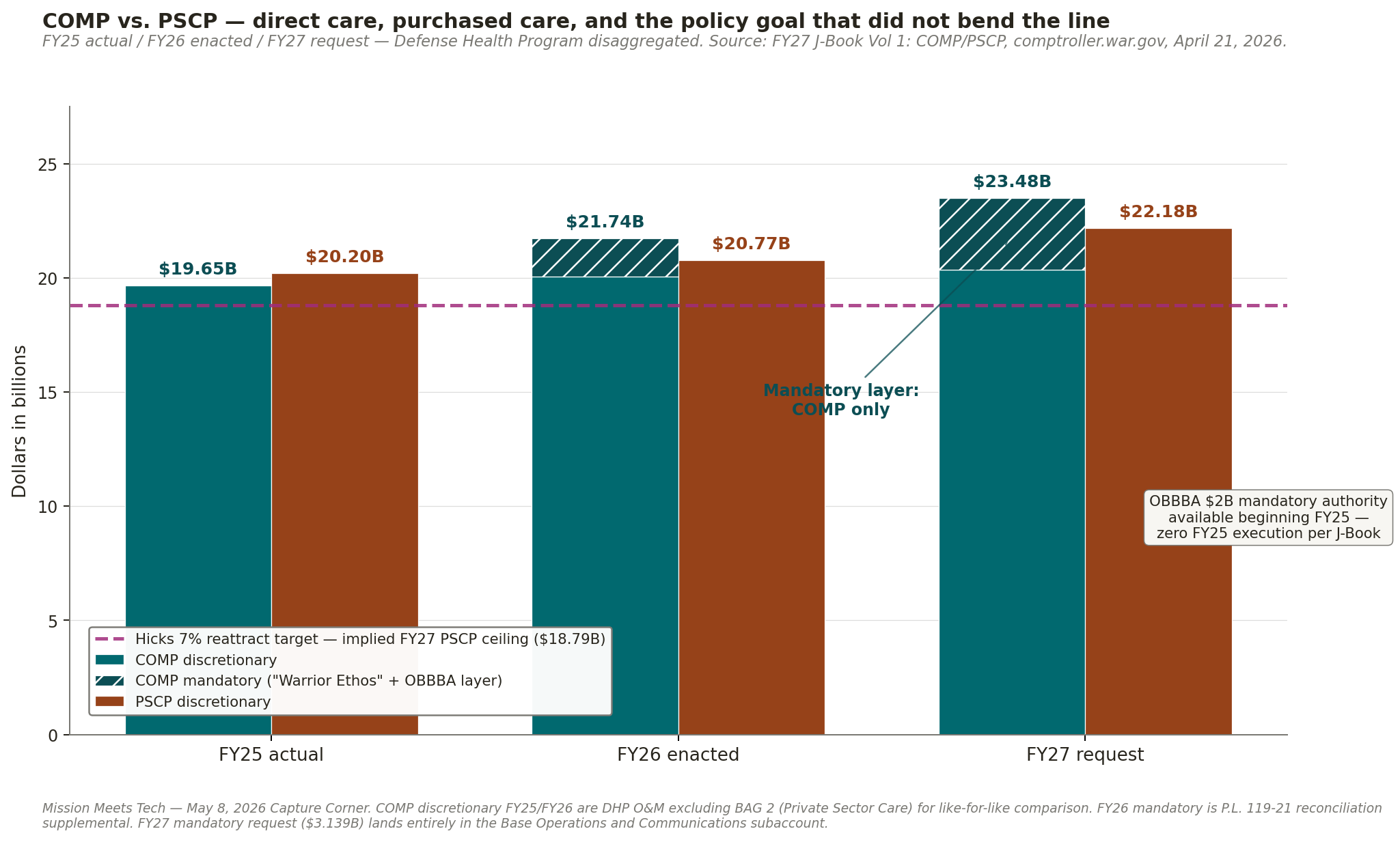
The dashed line is the implied FY27 PSCP ceiling if the Hicks 7 percent reattract goal had hit on schedule: $20.20 billion FY25 actual × 0.93 = $18.79 billion. Every actual and requested PSCP bar sits above the line. The gap between the line and the FY27 PSCP request is the policy commitment the budget request quietly retires.
The hatched stack on top of the FY26 and FY27 COMP bars is the mandatory layer. There is no PSCP equivalent. That asymmetry, visible in one image, is what the public-facing “transparency and accountability” framing does not name.
The Vendors and the Vehicles
The TRICARE managed care support contracts are the largest civilian-network purchase mechanism inside the new PSCP account. Both T-5 contracts are FY23-onward. Both have ceilings that run through the next decade.
T-5 East: Humana Government Business / Humana Military
- Contract: HT940223C0001
- Awarded: December 22, 2022 (DoD release announced T-5 East and West together at a $136 billion combined ceiling)
- Period of Performance: base year February 1, 2023 – January 31, 2024, plus eight one-year options through January 31, 2032, plus an 18-month phase-out
- Estimated total ceiling: $70.846 billion
- Type: Cost Plus Award Fee with FFP line items
- Solicitation: HT9402-20-R-0005
T-5 West: TriWest Healthcare Alliance
- Contract: HT940223C0002
- Awarded: December 22, 2022; reaffirmed April 2023 after Health Net Federal Services bid protest
- Health care delivery began: January 1, 2025, after a four-year transition
- Estimated total ceiling: $65.1 billion
- Six states moved East-to-West on January 1, 2025: Arkansas, Illinois, Louisiana, Oklahoma, Texas, Wisconsin (~1.5 million beneficiaries)
- Region: 26 states, ~5 million beneficiaries
- Health Net Federal Services lost the recompete, filed protest with GAO (denied August 4, 2023), then with the Court of Federal Claims (filed August 8, 2023). TriWest replaced HNFS as the West Region prime.
The combined T-5 ceiling, $136 billion over nine years, is the dominant capture surface inside PSCP. Whatever Congress does with PSCP in the FY27 cycle sets the rate-reset reference for the option-year exercises on both contracts.
TRICARE pharmacy: Express Scripts
The TRICARE pharmacy contractor is Express Scripts. Pharmacy is a separate large PSCP-flowing line. The formulary management and rate-setting workflow runs through the DOD Pharmacy and Therapeutics Committee with statutorily required Beneficiary Advisory Panel (BAP) comment. That workflow is currently in a state I’ll cover in detail in the BAP section below.
MHS GENESIS: Leidos Partnership for Defense Health (LPDH)
The MHS GENESIS prime is the Leidos Partnership for Defense Health: Leidos as lead, plus Accenture, Henry Schein One, and Oracle Cerner (Oracle Health), with about 35 supporting businesses. Original 2015 contract: $4.3 billion, expanded to roughly $5.5 billion to add Coast Guard and the VA baseline. The Department proposed a $1.4 billion sole-source extension in October 2024, with a three-year base of $1.13 billion plus a nine-month transition option of $263.3 million, to cover cloud migration. Open competition will not hit market until 2028 at the earliest. MHS GENESIS was declared fully deployed in March 2024. Today: 3,600+ DoD locations, 9.6 million patients, 194,000 clinical users, 100 percent of DoD garrison facilities. Currently deploying to the National Security Agency.
VA EHRM and FEHRM
The White House FY27 budget requests $4.24 billion for VA Electronic Health Record Modernization, with 26 new VA deployments planned in FY27 after a 13-site FY26 restart following a three-year deployment pause. The Federal Electronic Health Record Modernization (FEHRM) office is running a two-year cloud migration program (per CTO Lance Scott, June 2025).
The Mandatory-Floor Subaccount Story
This is the new fact MMT Premium subscribers need to anchor capture briefings around through the FY28 cycle.
The FY27 COMP mandatory request, $3.139 billion under the “Warrior Ethos” reconciliation bin, is not distributed across COMP. The J-Book line by line:
- In-House Care: $0 mandatory
- Consolidated Health Support: $0 mandatory
- Information Management: $0 mandatory
- Management Activities: $0 mandatory
- Education and Training: $0 mandatory
- Base Operations and Communications: $3,138,924 thousand ($3.139 billion)
- RDT&E: $0 mandatory
- Procurement: $0 mandatory
Base Operations and Communications is the subaccount that funds facility operations, utilities, data centers, the health IT network infrastructure at MTFs worldwide, and the communications systems that tie clinical operations together. Every dollar of the FY27 mandatory request lands here.
The FY26 precedent (P.L. 119-21 reconciliation supplemental) was $1.687 billion split across three subaccounts: Base Operations and Communications $887 million, In-House Care $700 million, Information Management $100 million.
The FY27 request:
- Concentrates the entire mandatory layer in Base Ops alone
- Escalates Base Ops mandatory by 3.5 times the FY26 mandatory level
- Requests the layer as recurring mandatory authority, not as a one-time emergency reconciliation
For capture: if your firm sells into the Base Ops subaccount, which funds facility operations, MTF physical plant, MTF-side network infrastructure, data centers, and health IT integration that flows through the facility budget rather than the GENESIS contract, the FY27 mandatory request is structural protection at a scale no other COMP line carries and no PSCP line carries at all. If your firm sells into clinical operations, education, or RDT&E at the MTFs and you assumed mandatory funding spread across COMP, your position is exposed to the FY26 → FY27 concentration shift.
The OBBBA $2 billion mandatory authority is the second mandatory layer. It became available beginning FY25. The J-Book table shows zero FY25 execution. The two layers route through different budget activity groups, and the J-Book does not connect them. The OBBBA layer is the unexecuted authority on the books. The Warrior Ethos layer is the FY27 ask.
Capture implication. Whatever the appropriators do with the Warrior Ethos request on June 11 sets the precedent on whether mandatory authority for direct-care infrastructure becomes recurring or stays exception-based. That precedent shapes every COMP capital plan from FY28 forward.
The CDMRP $1.5 Billion Decode
The Military Times May 5 reporting cited a “FY27 RDT&E down nearly $1.5 billion year-over-year” line. That phrasing carries the wrong implication for capture teams.
The COMP RDT&E FY27 request is $1.019 billion. The COMP RDT&E FY26 enacted is $2.473 billion. The net decrease is $1,453.3 million. The J-Book line item explicitly identifies the source: “$1,500.0 million decrease for FY 2026 one-time adjustments for Congressional Special Interest projects.”
This is the Congressionally Directed Medical Research Program (CDMRP). CDMRP has never been in the President’s Budget. CRS Insight IF10349 documents the structural fact: CDMRP “has not been part of the President’s budget request for DOW,” by design since 1992. Total CDMRP appropriations since FY1992 exceed $22 billion.
The recent CDMRP appropriations history:
- FY24: $1.509 billion across 38 research topics
- FY25: $650 million (P.L. 119-4 CR signed March 15, 2025), a 57 percent cut
- FY26: $1.27 billion across 34 programs (P.L. 119-75 signed February 3, 2026)
FY26 program detail: PRMRP $370M / 52 conditions, PRCRP $165M / 20 cancers, Breast Cancer $145M, Prostate Cancer $75M, Ovarian Cancer $50M, ALS $40M, Melanoma $40M, TBI $40M, Spinal Cord Injury $33M.
For capture: the FY27 RDT&E “cut” is not a programmatic cut to medical research. It is the same zero-out the President’s Budget submits every year for the line items Congress restores in mark-up. The Capture-relevant question is what HAC-D restores for FY27 CDMRP and at what topic mix. The TBI/psychological health, vision, hearing restoration, and orthotics/prosthetics topics that were eliminated in FY25 and partly restored in FY26 are the three watch-items for FY27 mark-up.
If your firm is positioned in CDMRP topics, do not brief leadership that the FY27 budget cuts medical research. Brief them that the FY27 budget submits the standard CDMRP zero-out and that the operative number is whatever HAC-D adds back on June 11. The amounts and topic mix are determined in subcommittee, ratified in Full Committee on June 24, and finalized in conference. The Senate has not announced its mark-up schedule.
The BAP Pause and What It Means for TRICARE Pharmacy
This is the under-reported operational fact MMT Premium subscribers need.
On March 10, 2025, the Secretary of Defense paused all DOD Federal Advisory Committees, including the Uniform Formulary Beneficiary Advisory Panel (UF BAP). The BAP made zero recommendations in FY2025 per the Federal Advisory Committee Act database. The Federal Advisory Committee Act database also confirms the BAP has issued 1,368 recommendations across its history.
10 U.S.C. §1074g requires BAP comment on Pharmacy and Therapeutics Committee recommendations before the DHA Director can sign the formulary determination. With the BAP paused, the workflow is statutorily blocked at the comment step.
Health.mil published guidance: “Until the UF BAP is re-established, the DOD P&T Committee meeting minutes are not available.” The delayed minutes window now spans:
- February 2025 P&T meeting: minutes delayed
- May 2025 P&T meeting: minutes delayed
- August 2025 P&T meeting: minutes delayed
- November 2025 P&T meeting: minutes delayed
- February 2026 P&T meeting: minutes delayed
- May 6-7, 2026 P&T meeting: held; minutes cannot release without BAP
The TRICARE formulary management workflow has been functionally frozen at the BAP-comment step for over a year. Express Scripts is operating against the formulary state as of the last released determination. Any formulary change pending from a P&T recommendation made in 2025 or 2026 is in queue waiting for either BAP reconstitution or a statutory workaround.
For pharmacy capture: the practical impact runs through three vectors. First, manufacturers seeking formulary additions or tier changes have a backlog of pending decisions with no announced clear-out date. Second, generics rotation and biosimilar adoption questions that normally process through quarterly P&T cycles are accumulating. Third, the FY27 PSCP pharmacy line is being requested under a formulary-management workflow that is currently non-operational at its statutory comment step.
The capture-relevant signals to watch: any Department announcement on UF BAP reconstitution; any Congressional language in the FY27 NDAA or Defense Appropriations Act addressing the workflow; any litigation seeking to compel formulary processing. If the FY27 NDAA or appropriations legislation directs reconstitution by a specific date, that is the inflection point for the formulary backlog.
What the Line Items Don’t Show
The COMP and PSCP architecture is being voted on in front of an operational record almost no capture brief is putting next to the budget arithmetic. Eight facts sit in primary-source documents from GAO, DOT&E, peer-reviewed clinical research, the VA OIG, NDAA report language, and the contractors themselves. Every one of them shapes capture positioning for the next 60 days.
The Hicks reattract goal expired unaddressed for the same reason any policy commitment expires unaddressed. The underlying systems could not deliver. The IT and contract-administration record around the FY27 COMP/PSCP architecture documents the operational reasons.
Direct-Care Side: MHS GENESIS
The patient portal. GAO May 2024 (MHS Genesis: Defense Health Agency Should Address Strategic Workforce, Patient Portal, and User Satisfaction Issues) found the MHS GENESIS patient portal has measured low user satisfaction. DHA does not have a strategic plan to address the gap. The portal is the front door for 9.6 million beneficiaries, and the user-experience surface for both COMP-side direct care and PSCP-side civilian-network referrals.
DOT&E operational suitability. The 2021 Director, Operational Test and Evaluation annual report found MHS GENESIS “was not operationally suitable largely because training and configuration management were unsatisfactory, dissemination of system change information was inadequate, and usability problems persisted.” DOT&E recommended a follow-on operational test and evaluation including patient-facing components and OCONUS sites. That FOT&E has not been completed. The FY24 DOT&E report on the RevX revenue cycle component is pending publication in 2QFY25.
Capture implication. When the Department or vendors describe MHS GENESIS as “fully deployed,” that statement covers fielding, not DOT&E suitability sign-off. The two are separate determinations. Any capture brief that conflates them is exposed.
Clinician usability and burnout. A peer-reviewed study (PMID 35925617) at an early MHS GENESIS adopter site measured System Usability Scale scores at 41 to 48 across the first post-Go-Live year, sustained below the 50 threshold typically classified as “not acceptable.” Self-reported clinician burnout stayed in the 26 to 37 percent range. Most clinicians wanted to return to the legacy EHR.
Capture implication. The reattract policy goal asked MTF clinicians to absorb additional direct-care load on a system measuring at “not acceptable” usability. The capacity ceiling is the EHR, not the staffing line.
Purchased-Care Side: T-5 Transition
The claims backlog. The January 1, 2025 T-5 West region transition produced a documented backlog of more than one million unprocessed claims in the early part of 2025. DHA spokesperson Peter Graves attributed the backlog to issues with “loading of provider files in their databases and claims systems.” Humana Military attributed East-region issues to “input of incorrect provider data.” In February 2025, Rep. Jen Kiggans (R-VA) warned the Defense Health Agency that the rollout was causing problems in the East region.
The TriWest software error. December 2025 TriWest Provider Pulse acknowledgment: PGBA, TriWest’s contracted claims processor, identified a “systems processing error” causing certain claims to be incorrectly processed as non-network instead of in-network. Recoupment efforts began November 24, 2025, with affected providers continuing to receive recoupment notices for 120 days afterward.
DHA performance reporting and downstream evidence. From July 2025 through March 2026, both contractors met contractually required standards (98 percent of claims within 30 days, 100 percent within 90 days). Beneficiary and provider experience reporting through Spring 2026 (Stars and Stripes May 3, 2026; North Carolina Health News April 25, 2026) describes patients flagged with “other health insurance” designations they do not have (blocking pharmacy coverage on prescriptions), providers leaving the TRICARE network citing claims-administration burden, individual unprocessed claims over $100,000, and 30 to 45 minute call wait times to TRICARE West customer service. TriWest reports serving 4.2 million members and processing more than 30 million claims since January 2025, with average processing time of eight days.
Provider directory accuracy. GAO 2024 review (covered by Military.com July 8, 2024): 85 percent of mental health provider listings in TRICARE East and 79 percent in TRICARE West had inaccuracies in location, gender, specialty, or contact information. Overall directory accuracy ran at 81 percent (HNFS) and 83 percent (Humana), both below the 95 percent contractual threshold.
Capture implication. Humana (T-5 East) and TriWest (T-5 West) are the dominant PSCP-side capture surface. Their contractually required performance thresholds were missed in the early T-5 ramp. The recoupment cycles and directory accuracy issues are the operational record any FY28 protest, rate negotiation, or option-year exercise will run against.
Congressional Track Running Alongside Mark-Up
The 2026 NDAA TRICARE directives. House Armed Services Committee 2026 NDAA report language directed the Department of Defense to deliver two reports to Congress by March 31, 2026 covering: root causes of TRICARE claim and payment delays (including contractor transitions, staffing shortages, and system inefficiencies); number of affected providers and beneficiaries (including disruptions in care, delayed authorizations, and access); performance metrics by region and contractor; reasons providers left the TRICARE network; and the full scope and impact of the T-5 contract implementation in TRICARE East and West.
The Comptroller General review. The U.S. Comptroller General is concurrently conducting a TRICARE contract transition review under Section 737 of the FY 2019 NDAA.
The provider association letters. July 2025 joint letters from APTA and other provider associations to the Senate Armed Services Committee and the House Armed Services Committee described a “crisis within the TRICARE system” citing “critical data transfer failure, rooted in flawed software implementation and deployment of an inaccurate database on a live platform, inflicting immeasurable damage upon providers and patients with no end point or solution.”
Capture implication. The Department’s responses to the NDAA-directed reports and the Comptroller General review will be on the record before the June 11 HAC-D mark-up. The PSCP $22.18 billion request lands in front of an oversight track that has documented operational concerns. Capture briefs that ignore this oversight surface are exposed. Government Affairs functions need read-ins on the Department’s report submissions specifically.
VA EHRM Coordination Risk
VA OIG patient-safety record. VA OIG Report 23-01450-114 (March 21, 2024), Electronic Health Record Modernization Caused Pharmacy-Related Patient Safety Issues Nationally and at the VA Central Ohio HCS in Columbus. Findings at VA Central Ohio HCS after April 2022 EHR deployment: previously-identified National Center for Patient Safety issues were a factor in 32 percent of facility pharmacy-related patient safety reports; EHR usability was a factor in 66 percent. The pharmacy backlog required a permanent 62 percent increase in clinical pharmacists. Pharmacy leaders had to create their own workarounds and education materials. Since April 2020, VA OIG has published 16 reports on the Oracle Cerner EHR, with nine relating to significant patient safety concerns.
Spokane VA harm record. Federal News Network and Spokane VA reporting: nearly 150 cases of patient harm identified at the Spokane VA hospital prior to the April 2023 deployment pause.
Software coding error. Fierce Healthcare February 20, 2024: Oracle Health software coding error transmitted incorrect VA Unique Identifier numbers from new-EHR sites to legacy VistA sites. Potential impact on 250,000 veterans. Manual medication safety checks were required at legacy sites.
The GAO recommendations backlog. GAO December 2025 update: VA has not fully implemented 16 of the 18 GAO recommendations on VA EHRM. 12 are designated priority recommendations because of their criticality to successful future deployments. Unimplemented priority recommendations cover cost estimating, schedule, program management, user adoption and satisfaction, and operational testing. VA delivered only a “notional schedule” to congressional committees, not the detailed cost estimate or schedule documentation Senate and House Authorizing and Appropriations Committees requested by September 30, 2025. GAO standing language: “Until VA fully implements the priority recommendations, future deployments risk prolonging management challenges like those experienced in the initial deployments and users will likely not be positioned to achieve optimal usage of the new electronic health record (EHR) system.”
Capture implication. The COMP and PSCP architecture asks MTF readiness and contracted-care delivery to grow against the same FEHRM-coordinated interoperability backbone that produced the Spokane and Columbus records. The VA’s accelerated 13-site FY26 / 26-site FY27 redeployment is moving forward against an open GAO recommendations backlog. If the FY27 NDAA or Defense Appropriations Act ties FEHRM funding or interoperability deadlines to VA EHRM milestones, the milestone risk is documented at the GAO-priority level. Capture teams positioning on FEHRM coordination work need an FY27 risk register that reflects this.
The Backbone
DEERS as single point of failure. When TriWest beneficiaries reported login errors in early January 2025, TriWest customer service told callers the issue was “back-end connectivity with DEERS [the Defense Enrollment Eligibility Reporting System].” DEERS is the master eligibility database determining TRICARE eligibility, prescription eligibility at retail pharmacies, claims processing routing, authorization letter generation, and home delivery prescription routing. DEERS is administered by DMDC under DoD Personnel and Readiness, with operational dependencies on DHA, the contractors (Humana, TriWest, Express Scripts), and every MTF and pharmacy network endpoint. The TriWest customer-service explanation in January 2025 pinpointed DEERS as the upstream dependency on which the T-5 backlog rode.
Capture implication. Every reform proposal that touches reattract execution, formulary timing, referral routing, or contractor performance flows through DEERS at some point in the workflow. DEERS modernization does not appear prominently in COMP/PSCP J-Book scope language because it sits in a different program lane (DMDC under USD(P&R)). The operational dependence is total. Capture teams positioning on TRICARE workflow improvements, MHS interoperability, or contractor performance solutions need DEERS-aware pipeline assumptions and a working understanding of the DMDC-DHA-contractor seam.
Putting It Together
The COMP/PSCP architecture is being voted on in front of an operational record that includes: an EHR not yet operationally suitable per DOT&E; a patient portal with measured low user satisfaction and no DHA strategic plan to address it; clinician usability scores below the “not acceptable” threshold for sustained periods; a million-plus claims backlog from the T-5 transition with continuing patient and provider impact through Spring 2026; an active Congressional investigation directed by the 2026 NDAA report language and a concurrent Comptroller General review; a VA EHRM with 16 of 18 GAO recommendations unimplemented and a documented patient-safety record; and a DEERS backbone that surfaces in every contractor disruption.
Capture teams using only the J-Book and the appropriations record are reading half the story. The other half is in the operational documentation cited above. The reattract goal did not bend the line because the systems behind the budget cannot deliver the appointment.
HAC-D 119th Congress Watchlist
The House Appropriations Defense Subcommittee marks up the FY27 Defense Appropriations Act on June 11. Full Committee follows on June 24. The 20-member subcommittee roster is the room where the FY27 COMP/PSCP product gets written.
Chair: Ken Calvert (R-CA)
Ranking Member: Betty McCollum (D-MN)
Vice Chair: Jake Ellzey (R-TX)
Republican members: Hal Rogers (R-KY), Steve Womack (R-AR), Robert Aderholt (R-AL), John Carter (R-TX), Mario Diaz-Balart (R-FL), Dave Joyce (R-OH), Chuck Fleischmann (R-TN), David Valadao (R-CA)
Democratic members: Marcy Kaptur (D-OH), Henry Cuellar (D-TX), Pete Aguilar (D-CA), Ed Case (D-HI), Susie Lee (D-NV), Joe Morelle (D-NY)
My read on the room (analytical projection, not voting record): Calvert has a long-standing track record on defense health funding decisions and on RDT&E disposition. McCollum is the senior Democratic appropriator on Interior-Environment but holds the Defense ranking position in the 119th and is the dominant Democratic voice on CDMRP topic disposition. Womack of Arkansas has constituent equities in CDMRP biomedical research. Carter of Texas, Diaz-Balart, and Calvert all have constituent equities in MTF infrastructure programs that would benefit from the Warrior Ethos Base Ops mandatory escalation. Government Affairs functions need member-by-member briefings ready to deploy by May 28 to be in the room before staff product-development closes.
Five-Point Exposure Assessment
Run this audit against every active task order, every IDIQ position, and every pipeline opportunity touching the Defense Health Program. Each point is binary: PASS or FAIL.
1. Account Mapping
Question: Have you mapped every active opportunity, every pipeline position, and every recompete in your defense health pipeline to the FY27 COMP or PSCP appropriation source?
Pass criteria: Every contract vehicle in your DHA pipeline tagged to the post-restructure account; each vehicle’s exposure to the COMP-side mandatory funding documented at the subaccount level (Base Operations and Communications versus other COMP subaccounts); capture team trained on the J-Book scope language for each account; internal appropriations tracking updated to reflect the new subcommittee dynamics.
Fail criteria: Pipeline still mapped to the legacy DHP single-account structure; “we assume our incumbent contracts roll over” without J-Book verification; BD team unaware of which subcommittee marks up which account; capture briefings still cite the FY26 enacted DHP as the operative budget reference.
Action for FAIL: Stand up the account-mapping audit this week. Use the COMP and PSCP J-Book as the authoritative scope reference. Tag every pipeline item to a specific appropriation source and, for COMP items, to a specific subaccount. October 1 is the deadline.
2. Mandatory Funding Concentration Awareness
Question: Does your capture team understand that the entire FY27 $3.139 billion COMP mandatory request lands in a single subaccount, Base Operations and Communications, and what that means for pipeline positioning?
Pass criteria: Internal brief documents the $3.139 billion FY27 mandatory request lands entirely in Base Operations and Communications; brief documents that every other COMP line carries $0 mandatory in FY27; brief documents the FY26 precedent ($1.687 billion split three ways) and the FY27 escalation (3.5x Base Ops alone, requested as recurring authority); brief documents the $2 billion OBBBA mandatory authority available beginning FY25 and the zero FY25 execution; capture team understands the J-Book does not connect the Warrior Ethos and OBBBA layers and routes them through different budget activity groups; pipeline assumptions on Base Ops-flowing programs reflect the protection; pipeline assumptions on non-Base-Ops COMP programs and on PSCP-flowing programs reflect the absence of a mandatory backstop.
Fail criteria: Pipeline assumes the COMP mandatory layer spreads across direct care broadly; capture brief conflates the two mandatory authorities without naming the Base Ops concentration; capture brief misses the FY25 zero-execution fact.
Action for FAIL: Brief leadership on the subaccount concentration. The Warrior Ethos request is the structural protection for facility operations, MTF network infrastructure, and the data centers underneath the MHS technical estate. The asymmetry survives across Congresses unless deliberately changed.
3. CDMRP Decoding
Question: Does your capture team understand that the FY27 RDT&E decline is the standard CDMRP zero-out, not a programmatic cut, and have they identified which CDMRP topic mix HAC-D is likely to restore?
Pass criteria: Internal brief identifies the $1.5 billion decline as the President’s Budget zero-out for Congressional Special Interest projects; brief documents the CDMRP appropriations history (FY24 $1.509B, FY25 $650M, FY26 $1.27B); brief identifies which CDMRP topics are positioned for restoration in FY27 mark-up (TBI/psychological health, vision, hearing, orthotics/prosthetics: the FY25 eliminations partly restored in FY26); pipeline reflects topic-level positioning, not topline RDT&E exposure.
Fail criteria: Capture briefings treat the FY27 RDT&E line as a programmatic cut; no internal map of which CDMRP topic equities map to which HAC-D members; pipeline assumes the FY27 PB number is the operative funding reference for medical research.
Action for FAIL: Brief leadership on the CDMRP zero-out pattern. Map your firm’s medical research equities to specific HAC-D members. Engage trade associations on CDMRP topic positions before May 28.
4. House Mark-Up Exposure
Question: Is your government affairs team positioned to track and respond to both the HAC-D subcommittee mark-up on June 11 and the Full Committee mark-up on June 24?
Pass criteria: Both mark-up dates on the calendar at the leadership level; specific COMP and PSCP line items in your pipeline flagged for amendment exposure; member-by-member briefings ready for the 20 HAC-D members; public position on the COMP and PSCP architecture developed and ready to deploy; trade association sign-on positions reviewed and locked before the subcommittee step.
Fail criteria: Mark-up dates not on the leadership calendar; no firm position on whether your firm supports, opposes, or is neutral on the architecture; Government Affairs not engaged with HAC-D subcommittee staff; “wait and see what the bill says” posture; sign-on letters held until after June 11.
Action for FAIL: Engage now. Trade associations are coordinating positions. The dispositive vote on PSCP line items typically lands at the June 11 subcommittee step. Full Committee on June 24 typically ratifies the subcommittee product with limited amendments. Sign-on letters and member positions need to be locked before May 28 to be in the room before staff product-development closes. After Full Committee, the negotiating room is the conference committee, and that is a smaller room with fewer seats.
5. BAP Pause and Pharmacy Workflow
Question: If your pipeline touches TRICARE pharmacy or the formulary management workflow, does your capture team understand the BAP pause and its implications for FY27 pharmacy positioning?
Pass criteria: Internal brief documents the March 10, 2025 SecDef pause on Federal Advisory Committees including UF BAP; brief documents the statutory dependency under 10 U.S.C. §1074g; brief documents the delayed P&T minutes window from February 2025 through May 2026; capture team is tracking any signal of UF BAP reconstitution or statutory workaround; pipeline assumptions reflect the workflow pause where pharmacy capture depends on formulary timing.
Fail criteria: Capture briefings treat formulary management as operating normally; no tracking of UF BAP reconstitution signals; pricing assumptions on formulary changes assume normal P&T cycle disposition.
Action for FAIL: Brief leadership on the BAP pause. Add UF BAP reconstitution tracking to the capture intelligence brief. Coordinate with Express Scripts contacts on the formulary backlog state.
Live Signal Watchlist
Signal 1: HAC-D Subcommittee Mark-Up, June 11
MMT Projection: High Confidence
The dispositive vote on FY27 COMP and PSCP line items lands here. Watch for: bill text on COMP scope and PSCP scope, committee report language directing reporting requirements, any amendment that touches the Warrior Ethos Base Ops mandatory request, CDMRP topic restorations, and any directive language on the reattract goal.
Action: Have member-by-member briefings ready by May 28. Flag bill text for capture relevance within 24 hours of the June 11 product. Brief leadership the same day.
Signal 2: Full Committee Mark-Up, June 24
MMT Projection: High Confidence on Ratification, Medium Confidence on Amendment Volume
Full Committee typically ratifies the subcommittee product with limited amendments. Watch for: any amendment that touches the structural questions the subcommittee did not settle, any directive language added at Full Committee level, any reporting requirements specific to the COMP and PSCP architecture.
Action: Position to respond to amendments within 24 hours. Conference committee is the next room and the smallest one.
Signal 3: Senate Defense Appropriations Timing
MMT Projection: Medium Confidence on Timing, High Confidence on Direction
The Senate has not announced its mark-up schedule. Senator McConnell’s questions about the reconciliation strategy for the $350 billion supplemental piece may slow the regular-order appropriations track. The Senate’s posture on COMP and PSCP is not yet articulated publicly.
Action: Government Affairs in inquiry mode with Senate subcommittee staff now.
Signal 4: MHS Oversight Hearing Reschedule
MMT Projection: Medium Confidence
The cancelled March 25 hearing has not been rescheduled as of May 7. The Houlahan letter raises the political cost of further delay. A rescheduled hearing in the May to July window is plausible. A continued cancellation through the appropriations cycle is also plausible.
Action: Add to capture intelligence brief. The witness list itself will be a signal about the reattract goal status.
Signal 5: UF BAP Reconstitution
MMT Projection: Low Confidence on Timing, High Confidence on Direction
The DOD Pharmacy and Therapeutics formulary workflow is statutorily blocked at the BAP-comment step. Some path forward, whether reconstitution, statutory workaround, or workflow exception, is required for formulary management to resume normal disposition. The form and timing of that path are open.
Action: Add UF BAP reconstitution tracking to the capture intelligence brief if pharmacy capture is in your portfolio.
Signal 6: FY28 PB Submission Posture
MMT Projection: High Confidence on Direction
The FY28 President’s Budget submission, expected February-March 2027, will reflect whatever Congress did with COMP and PSCP in the FY27 cycle. Watch for: whether Warrior Ethos mandatory recurs, whether OBBBA execution catches up, whether any new account structures appear, and any service-level signals on medical readiness funding posture.
Action: Position pipeline assumptions to absorb either continuation of the FY27 trajectory or a rate-reset reattract revival. Build both scenarios into FY28 capture briefs.
Capture Implications by Account
Highest PSCP Exposure
TRICARE T-5 East: Humana Government Business (HT940223C0001). $70.846 billion ceiling through January 31, 2032. PSCP growth in FY27 sets the rate-reset reference for the next option-year exercise. Humana’s incumbent position is structurally protected through the option-year mechanism but exposed to any Congressional rate-restraint signal in the FY27 mark-up product.
TRICARE T-5 West: TriWest Healthcare Alliance (HT940223C0002). $65.1 billion ceiling. Health care delivery began January 1, 2025, the first year of full-region operation. TriWest’s incumbent position is on a steeper utilization-versus-ceiling ramp than Humana’s.
TRICARE pharmacy: Express Scripts. Pharmacy is one of the larger PSCP-flowing programs. Formulary and rate dynamics shape the incumbent negotiating position. The BAP pause is the operational fact governing any formulary change pending from a 2025 or 2026 P&T recommendation.
Civilian-network access expansion programs. Any program designed to expand civilian-network access under MISSION Act-equivalent statutory authority will run through PSCP.
Highest COMP Exposure: Base Operations and Communications Subaccount
MTF facility operations and physical-plant programs. The FY27 $3.139 billion mandatory layer lands here. Incumbents on facility upgrade work, MTF physical plant, and base-services contracts at MTFs are positioned in the protected layer.
MTF-side network infrastructure and data centers. The Base Ops subaccount funds the network infrastructure and data centers that sit beneath the MHS technical estate. Incumbents on this work are inside the mandatory protection.
MHS GENESIS deployment phases that flow through Base Ops. Where GENESIS deployment work routes through facility-side budget rather than the LPDH contract directly, those phases are inside the Base Ops mandatory protection. Capture teams need to verify which deployment workstreams sit on which side.
Highest COMP Exposure: Other Subaccounts (Discretionary Only)
In-House Care, Consolidated Health Support, Information Management, Education and Training. All carry $0 mandatory in FY27. These programs are discretionary-only inside COMP and exposed to the same FY28 risk that PSCP carries.
Medical RDT&E. The COMP RDT&E request is $1.019 billion. Incumbents in CDMRP topics are dependent on what HAC-D restores on June 11. The capture-relevant question is the topic mix.
Cross-Account Exposure
MHS GENESIS: Leidos Partnership for Defense Health. The clinical platform straddles direct care delivery and network interoperability. The $1.4 billion sole-source extension proposed October 2024 is the bridge to the 2028 open competition. Capture teams need to understand which deployment phases ride on which subaccount.
FEHRM. The Federal Electronic Health Record Modernization office operates across the VA and DoD interoperability boundary. Funding flows are mixed across accounts and across departments. Pursuit teams need account-specific awareness.
VA EHRM. The $4.24 billion FY27 request is in the VA budget, not the DoD budget. But the FEHRM coordination requirement means VA EHRM deployments and MHS GENESIS deployments share interoperability infrastructure capture surface.
Bottom Line Assessment
The COMP and PSCP split is the budget catching up to obligation behavior. The Pentagon was already the second-largest contracted-medicine buyer in the federal government before the restructure. The restructure makes the obligation visible, not larger.
What it changes for capture: the appropriations dynamics that drive different programs now run through different accounts with different political pressures. The COMP-side mandatory funding lands entirely in one subaccount, Base Operations and Communications, and that subaccount becomes the structural-protection capture surface for the next two budget cycles. The reattract goal expires unaddressed at the end of this calendar year. Whatever the Department says about that goal between now and the FY28 submission shapes whether FY27 looks like the new normal or the high-water mark for PSCP rate growth.
Winners: Incumbents in MTF physical plant, facility operations, MTF-side network infrastructure, and data center work that routes through Base Operations and Communications. Humana and TriWest on T-5 (incumbent rate protection through option-year mechanisms). LPDH on MHS GENESIS through 2028. Capture teams that map pipeline to the new account structure and the subaccount concentration within the first 90 days. Trade associations that build positions on COMP and PSCP scope before May 28.
Losers: Incumbents on PSCP-flowing managed care positions that treat the FY27 growth rate as the FY28 baseline without tracking the reattract gap. Pipeline shops still mapped to the legacy DHP single-account structure. Pursuit teams that briefed leadership the FY27 RDT&E “cut” as a programmatic decline rather than the standard CDMRP zero-out. Pharmacy capture briefings that miss the BAP pause. Government Affairs functions not engaged with HAC-D subcommittee staff before May 28.
Strategic imperative: The split is the structural fact for the next two budget cycles. Pipeline maps need to reflect it down to the subaccount level on the COMP side. Government Affairs engagement needs to reflect the 20-member HAC-D roster member by member. Capture timing needs to reflect the June 11 subcommittee mark-up, the June 24 Full Committee mark-up, the Senate timing question, the reattract goal status, the BAP reconstitution question, and the FY28 PB submission. The window between now and December 31 is the period in which the Department has to say something or not say something about the policy commitment that justified the entire reattract architecture. What gets said, or not said, locks in the FY28 capture environment.
The accounting is catching up. The behavior is settled. The mandatory floor lives in one subaccount. The policy commitment is the variable.
Let’s roll.
— Mary
Mission Meets Tech