Two of Forty-Six
The military built a precise way to measure whether its surgeons are ready for war. Last year it checked one specialty against the bar. Two of forty-six active-duty neurosurgeons cleared it. A GAO report this month points to why the fix has been hard to manage: the Department of War cannot yet count the civilian partnerships built to close that gap. The department named the right mission and accepted the roadmap. Friday, the part that should give everyone hope: the fix is already proven, and half of it is running inside the military's own networks.
Friends,
A military surgeon is ready for combat when the caseload says so. Enough trauma, enough critical patients through the hands, and the skill holds. Stop, and it fades. Every surgeon knows this, and in 2019 the Defense Health Agency built a metric around it.
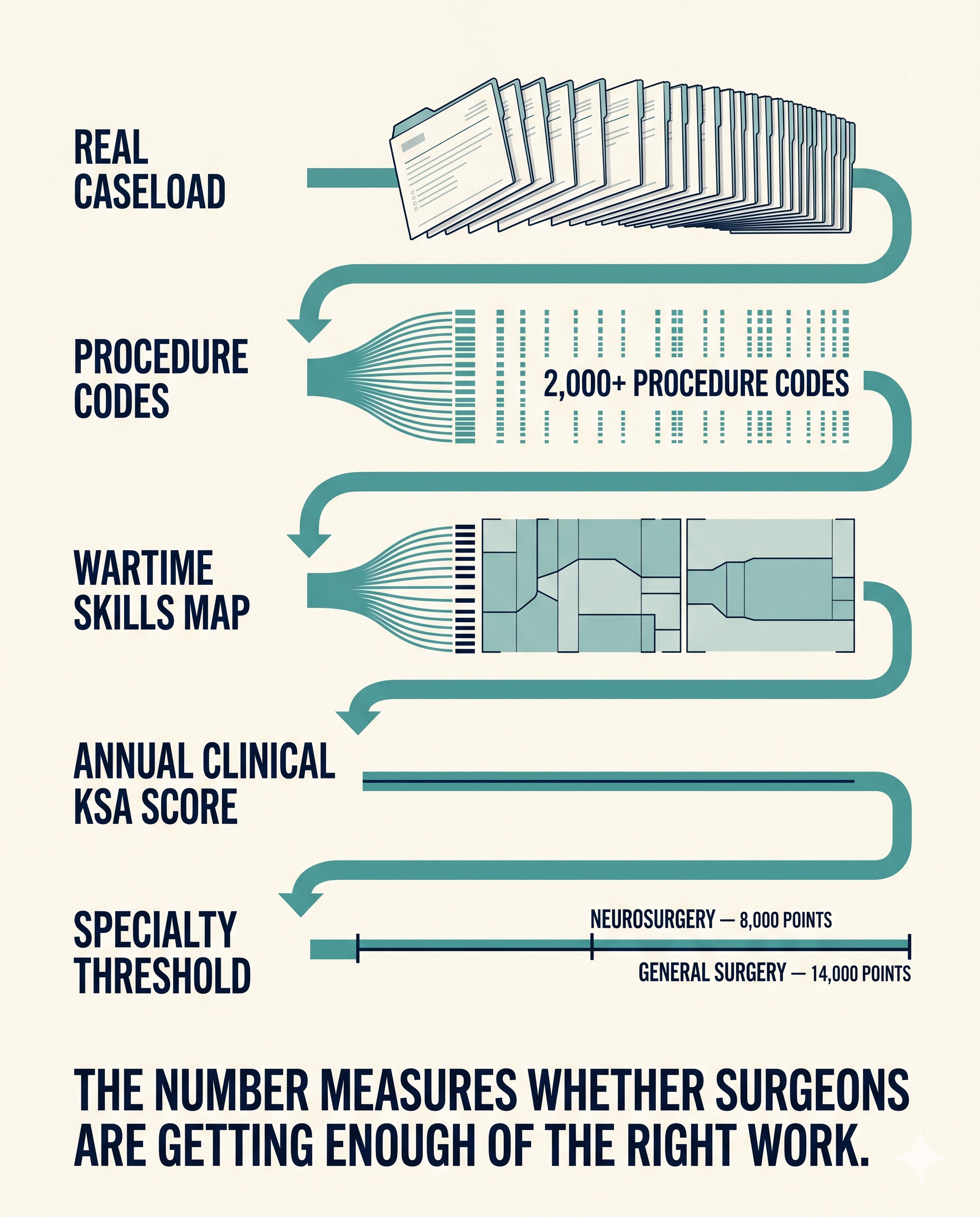
The agency, working with the American College of Surgeons and the Uniformed Services University, told its wartime specialties to measure readiness directly, so skill decay would show up on a chart before it showed up on a casualty. The method is sharper than most people outside military medicine realize. A consortium of trauma surgeons defined the specific skills a deployed surgeon needs, several hundred of them, and mapped each to the procedure codes that build it, more than two thousand codes in all. Run a surgeon's real caseload through that map and you get one annual number, the clinical KSA score, benchmarked to the volume a deployed surgical team handled in the busiest year of the recent wars. For a general surgeon, the readiness threshold is fourteen thousand points a year. For a neurosurgeon, eight thousand. In a single figure, the score says whether a surgeon is doing enough of the right work to be trusted with a casualty.
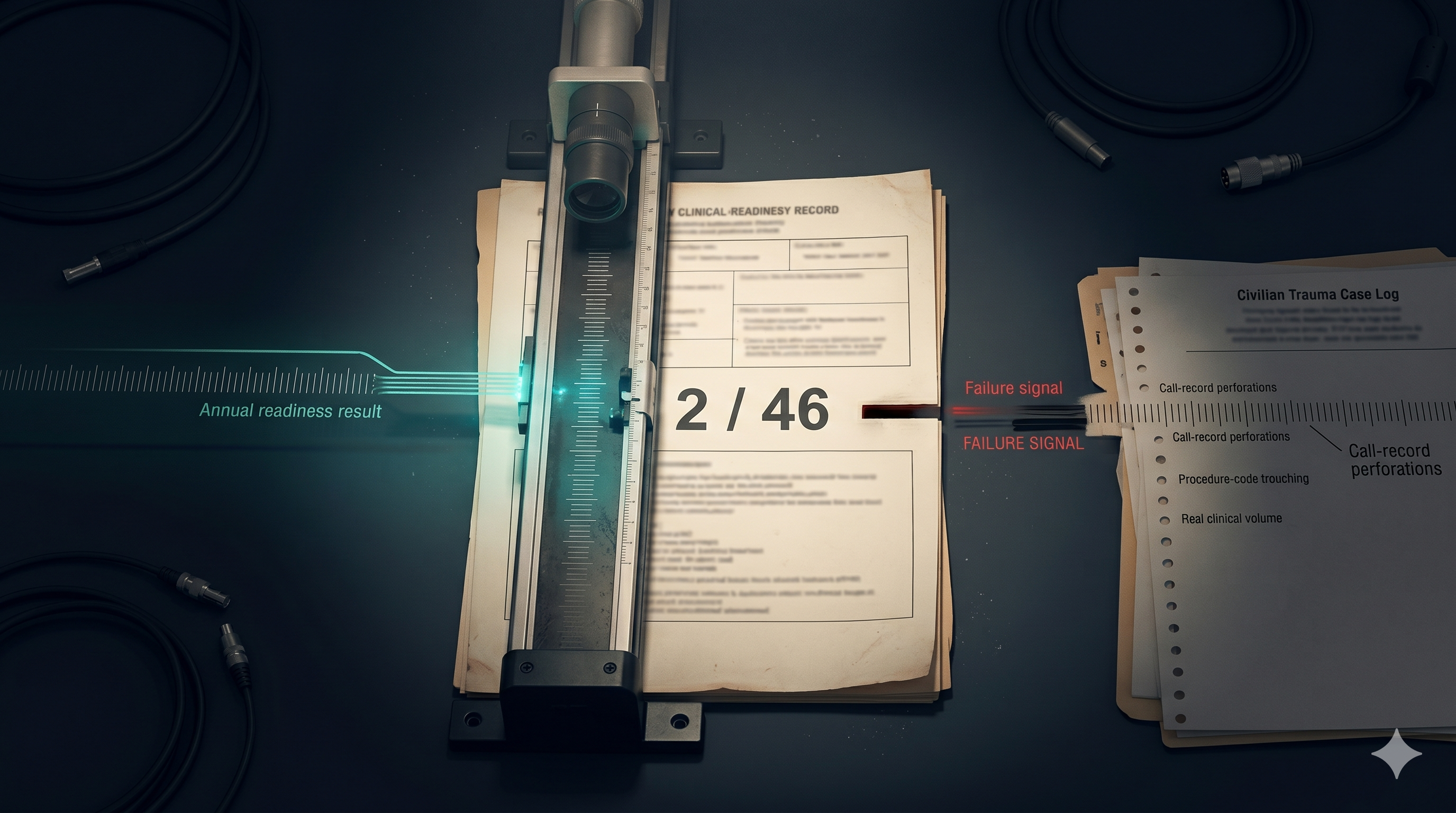
Last year a study in Military Medicine checked one specialty against its bar.
Forty-six active-duty neurosurgeons. Two cleared it.
That number is not an indictment of anyone in uniform. It is a volume problem, and the same study confirmed the bar is fair and reachable. Neurosurgery is not alone either. A 2021 study in JAMA Surgery ran the same analysis across general surgery and found the share of military general surgeons meeting the fourteen-thousand-point threshold fell from 16.7 percent in 2015 to 10.1 percent in 2019, while surgical volume inside military hospitals dropped about a quarter. About one in ten by 2019, down from one in six four years earlier. Across two very different specialties, the metric tells the same story, and it is the story the metric was built to catch.
The fix is known: send surgeons where the cases are. The military built infrastructure to do exactly that. Which brings us to the report.
What GAO found, and the shape of the work
On June 4 the Government Accountability Office published its review of those partnerships. The finding is plain. The Department of War cannot yet say how many it has. Inventory efforts across the services have been ad hoc. There is no complete, current count, and no department-wide rule for collecting the clinical-activity data that would show what a surgeon actually did inside a partner hospital, or whether it moved the readiness number.
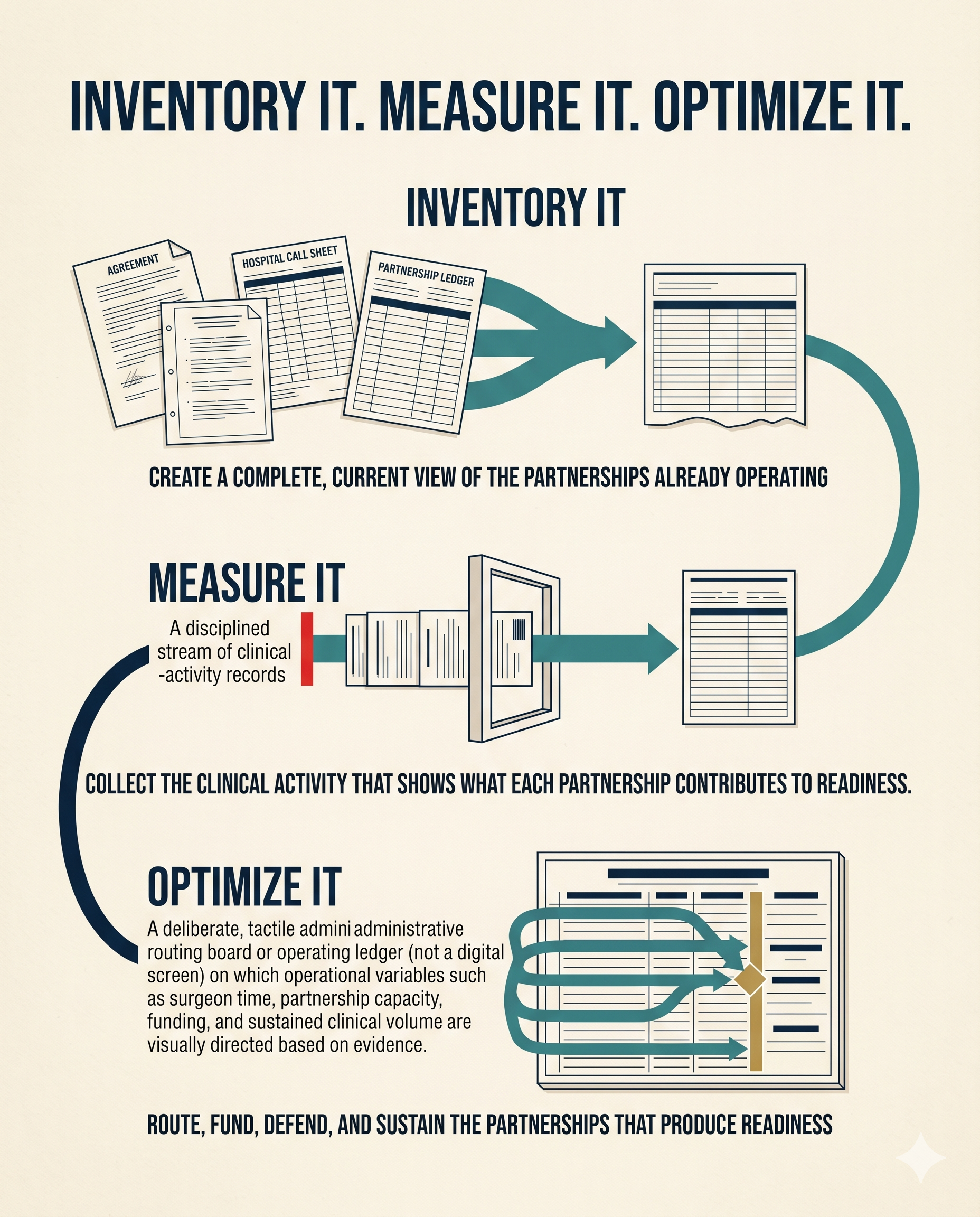
GAO made nine recommendations, and read together they describe the shape of the work rather than a scolding. The first asks the department to build a standardized way to inventory partnerships and to use one vehicle in particular, the External Resource Sharing Agreement, to cut cost while increasing readiness. The next asks each service, Army, Navy, and Air Force, to inventory its own partnerships. The third asks each service to assess what those partnerships actually contribute to readiness. The last asks the department to issue guidance for collecting complete clinical-activity data in the specialties that have readiness metrics. Inventory it. Measure it. Optimize it. That is the sequence.
The department concurred with seven recommendations and partially concurred with two. That response is the part worth holding onto. An institution that agrees with the diagnosis is one ready to act on it. The report is not a verdict. It is a roadmap, and the department signed for most of it.
The idea under all nine is one line. You strengthen what you can measure. The work ahead is building the measurement.
The system built to fix this, and the right way to run it
The partnerships exist because military hospitals stopped seeing enough trauma to keep their surgeons sharp, and that is physics, not failure. When a hospital's operating rooms go quiet, the surgeons inside them lose reps they cannot get back any other way.
The infrastructure built to replace those reps is real, named, and already running. The Air Force sustains trauma skills through its Centers for Sustainment of Trauma and Readiness Skills, embedded in civilian hospitals, the largest at the R Adams Cowley Shock Trauma Center in Baltimore, with others in cities like Cincinnati and St. Louis. The Army runs its Trauma Training Center at Ryder Trauma Center in Miami. The Navy runs its Trauma Training Center at Los Angeles General. Behind those sit dozens more enduring partnerships, roughly three dozen civilian training programs across about twenty-five institutions where military physicians keep their hands in high-volume medicine. The legal plumbing is the External Resource Sharing Agreement under title 10, along with memoranda of understanding and training affiliation agreements, the instruments that let an active-duty surgeon take real call inside a civilian trauma bay.
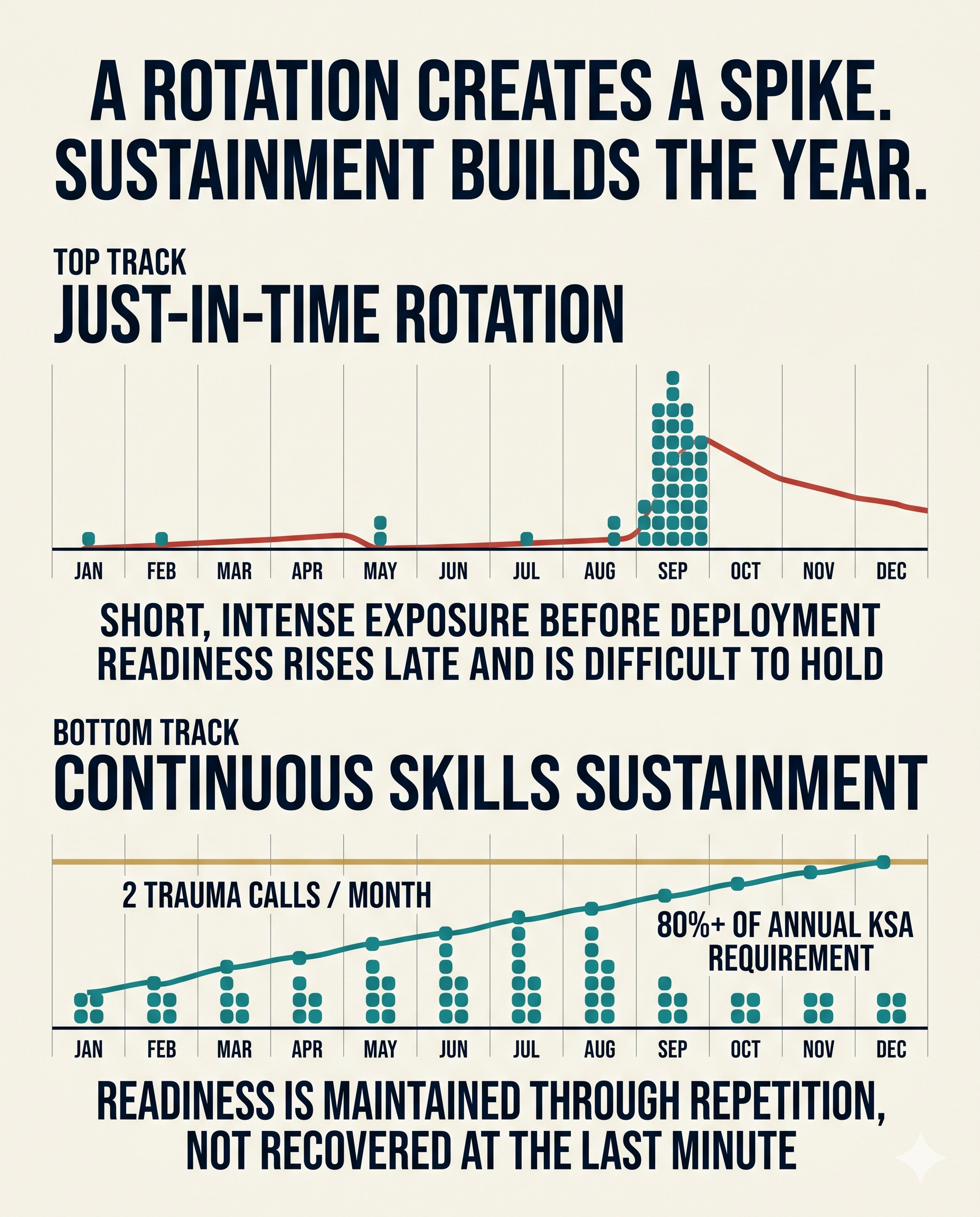
There is a right way and a wrong way to use all of it, and the literature is clear on which is which. Most partnerships run on a just-in-time model, a short and intense rotation right before a deployment. The stronger model is skills sustainment, regular trauma call at steady intervals all year. One Navy study embedded general surgeons in an urban level-1 trauma center taking two calls a month and found they generated more than eighty percent of the KSA points a full year of readiness requires, most of them in exactly the combat-relevant cases that matter. The mechanism works when it runs continuously. The task GAO named is being able to see all of it at once, well enough to run it that way on purpose.
Why the timing is different this time
Surgical skill has always softened between wars. British surgeons named it the Walker Dip, after the Royal Navy surgeon who described the loss of hard-won trauma proficiency in quiet years. American surgeons saw the same after Iraq and Afghanistan and called it the Peacetime Effect. Every generation meets it. What is different now is what waits on the other side.
The last two wars were fought under air superiority, with fast evacuation and the golden hour. A wounded service member could often reach a surgeon within the hour, and the case-fatality rate held near nine to ten percent in part because of it. Planners do not expect that against a peer. They expect contested skies, delayed evacuation, and what the doctrine calls prolonged field care: holding a casualty alive far forward for hours or days, not minutes, because the ride out is not coming on schedule. Army modeling for the Indo-Pacific projects casualty rates well above the recent wars. In that fight, the surgeon who was ten percent ready against a golden-hour standard is asked to do more, with less behind them, for longer. The readiness premium rises exactly as the cushion that hid the gap falls away.
The department is already moving
None of this is news to the people running military medicine. They are already acting on it from several directions at once.
The Department of War seated a new DHA director in February. Vice Admiral Darin Via, formerly the Navy surgeon general, opened by naming the agency's job in one line. "The Defense Health Agency, in its entirety, is a combat support agency." Warfighter medical readiness, he said, is the point of the enterprise. In May, the new assistant secretary of war for health affairs, Keith Bass, told a worldwide audience of military health professionals the same thing in different words. Medical readiness is what supports lethality, and the department has been making deliberate investments in the blood program, the Joint Trauma System, research, and medical logistics to back it.
The volume problem itself is already named at the top. After years of steering beneficiaries out to the civilian network, which is what emptied the operating rooms in the first place, the department directed the system to re-attract a share of those patients to military hospitals by the end of 2026, to rebuild the case volume its surgeons need. Execution has been the hard part, and it is the open question. The intent reads the problem correctly, and it carries a second benefit the readiness studies flagged. Every patient cared for inside a military hospital instead of purchased outside it is both a readiness rep gained and a purchased-care dollar saved. Readiness and cost point the same direction here, which is exactly what GAO's first recommendations ask the department to chase.
Read against all of that, the GAO report is not a contradiction of the mission. It is the measurement layer the mission has been missing. The director names where the agency is going. The review maps the work between here and there. They agree.
What closing the gap is worth
We can account for nearly everything else that moves toward a fight. Every round downrange. Every rotor hour. Every unit of blood headed to a casualty collection point. The logistics enterprise can find a single pallet across an ocean tonight.
Bringing that same clarity to the hospitals that keep a surgeon ready is the gap worth closing next.
The work is concrete, and so is what it unlocks. A partnership the department can see is one it can fund with confidence, defend in a budget review, route surgeons through deliberately, and reinforce before it frays. GAO's ninth recommendation asks for the clinical-activity data system that would make all of that real. The department concurred. The path runs through measurement first, and it is open. For anyone watching this space, the signal to track is simple. Who builds the system that finally lets the department count clinical activity inside its partnerships, because the routing, the funding, and the budget defense all wait on it.
Friday's issue is about why this is solvable rather than daunting. The military is not staring at a blank page. The fix is already proven in two places. One is the American civilian health system, which met the same volume problem in its rural hospitals and mapped the way out. The other is closer to home: the military's own tele-critical care network, which already runs the exact model the surgical side needs. Friday I will put both on the table and show how they fit. The destination is set. The route is already drawn.
The person at the end of the number
Strip away the report and the metric and one thing remains. A wounded service member, somewhere forward, in a year we have not reached, with minutes that matter.
The undersecretary of war for personnel and readiness put it plainly at that same conference in May. Everything the giant medical enterprise does, he said, comes down to the tip of the spear, where a medic with an aid bag has to apply lifesaving measures to someone who is wounded. The surgeon who receives that casualty an hour or a day later is one the system worked to keep ready. Whether that surgeon has the reps was decided years earlier, in peacetime, by whether the partnership that supplies the volume existed, worked, and could be counted.
Two of forty-six is why this matters. The GAO roadmap is how we close it. We do the work now so the person on the table gets the surgeon the mission promised them.
That is the whole point, and it is worth getting right. On Friday, the proof that we already know how.
Let's roll.
— Mary
Mission Meets Tech
The views expressed in this newsletter are my own and do not represent the official position of any organization. This content is for informational purposes only.
MMT Premium
This is Part 1 of a two-part series. Friday brings the civilian mirror, the network the military already built, and the operational telehealth that pairs with it. Premium subscribers get the companion Capture Corner with this issue: the nine GAO recommendations read as a roadmap, the live vehicles already moving against this gap, and the case for why building the Department of War's clinical-activity data layer is the work that supports everything downstream of it.
Founding Member rate: $199/year, locked permanently for the first 100 subscribers. Standard rate: $249/year or $29/month.
Premium adds 48-hour early access to deep-dive analysis, monthly Capture Intelligence Sheets with sourced action windows, direct Q&A access (reply to any premium issue), and tool discounts: ProposalPulse $14.99 per assessment, MarketPulse $35 per brief.
Subscribe at missionmeetstech.com/pricing.
Sources
[1] Government Accountability Office, GAO-26-107677, "Defense Health Care: Actions Needed to Assess Civilian Partnerships' Contributions to Readiness," published and released June 4, 2026 (the department does not know the total number of partnerships department-wide; inventory efforts ad hoc; no department-wide guidance for collecting complete clinical-activity data; nine recommendations, seven concurred, two partially concurred). https://www.gao.gov/products/gao-26-107677
[2] Dewar et al., "Optimizing Military Neurosurgery Readiness and Validation of the Knowledge Skills and Abilities Metric Threshold," Military Medicine, Vol. 191, Issue 3-4, March/April 2026, pp. e827-e833 (46 active-duty attending neurosurgeons, CY2022; two reached the 8,000-point annual KSA threshold; threshold validated as reasonable and attainable; current MTF volume does not support wartime readiness as described by the metric). https://academic.oup.com/milmed/article/191/3-4/e827/8262724
[3] Dalton et al., "Analysis of Surgical Volume in Military Medical Treatment Facilities and Clinical Combat Readiness of U.S. Military Surgeons," JAMA Surgery, 2021 (share of military general surgeons meeting the 14,000-point KSA threshold fell from 16.7% in 2015 to 10.1% in 2019; military hospital surgical volume down roughly 25%). https://pmc.ncbi.nlm.nih.gov/articles/PMC8552115/
[4] USU / American College of Surgeons, Knowledge, Skills, and Abilities (KSA) Clinical Readiness Program (consortium-defined wartime KSAs mapped to more than 2,000 CPT codes; general-surgeon readiness threshold of 14,000 points, set at the 70th percentile of deployed surgical-team volume in 2011). https://www.newswise.com/articles/ksa-metrics-will-improve-military-surgeons-readiness
[5] Ruggero et al., "Initial Assessment of a Regional Military-Civilian Partnership on Trauma Surgery Skills Sustainment," Military Medicine, 2023 (a military surgeon taking two trauma calls per month over 12 months generates more than 80% of the KSA points required to meet the deployment-readiness threshold; 14,000-point general-surgeon threshold; only about 9% of military surgeons currently meet it). https://pubmed.ncbi.nlm.nih.gov/35880592/
[6] Defense Health Agency, "'We Are a Combat Support Agency,' says new DHA Director," February 12, 2026 (Vice Adm. Darin K. Via assumed the DHA director role February 2, 2026). https://www.dha.mil/News/2026/02/12/18/57/We-Are-a-Combat-Support-Agency-says-new-DHA-Director
[7] Health.mil / DVIDS, "Military medicine is a 'no-fail mission,' says Department of War top military health leader," May 27, 2026 (Assistant Secretary of War for Health Affairs Keith Bass on medical readiness, lethality, and strategic investments in the blood program, Joint Trauma System, research, and medical logistics; Undersecretary Anthony Tata on the tip of the spear). https://www.health.mil/News/Articles/2026/05/27/Military-medicine-is-a-no-fail-mission-says-Department-of-War-top-military-health-leader
[8] Navy Times, reporting on the Defense Health Program budget and the effort to re-attract beneficiaries to military hospitals to rebuild case volume, 2026. https://www.navytimes.com/pay-benefits/military-benefits/health-care/2026/05/05/defense-department-proposes-splitting-military-health-system-budget/
[9] "To Conserve Fighting Strength in Large-Scale Combat Operations," Military Review, 2025 (Indo-Pacific casualty projections; prolonged evacuation; prolonged field care). https://www.armyupress.army.mil/journals/military-review/online-exclusive/2025-ole/conserve-fighting-strength-in-lsco/
[10] Congressional Research Service, "Defense Primer: Military Health System," IF10530 (FY2017 NDAA civilian partnership authorities; External Resource Sharing Agreement authority). https://www.congress.gov/crs-product/IF10530