The Workflow Was Designed to Deliver
A credentialed third party generated evidence before the read. Twenty-one years later, that is the architecture CMS is shutting other modalities down for not having.
Friends,
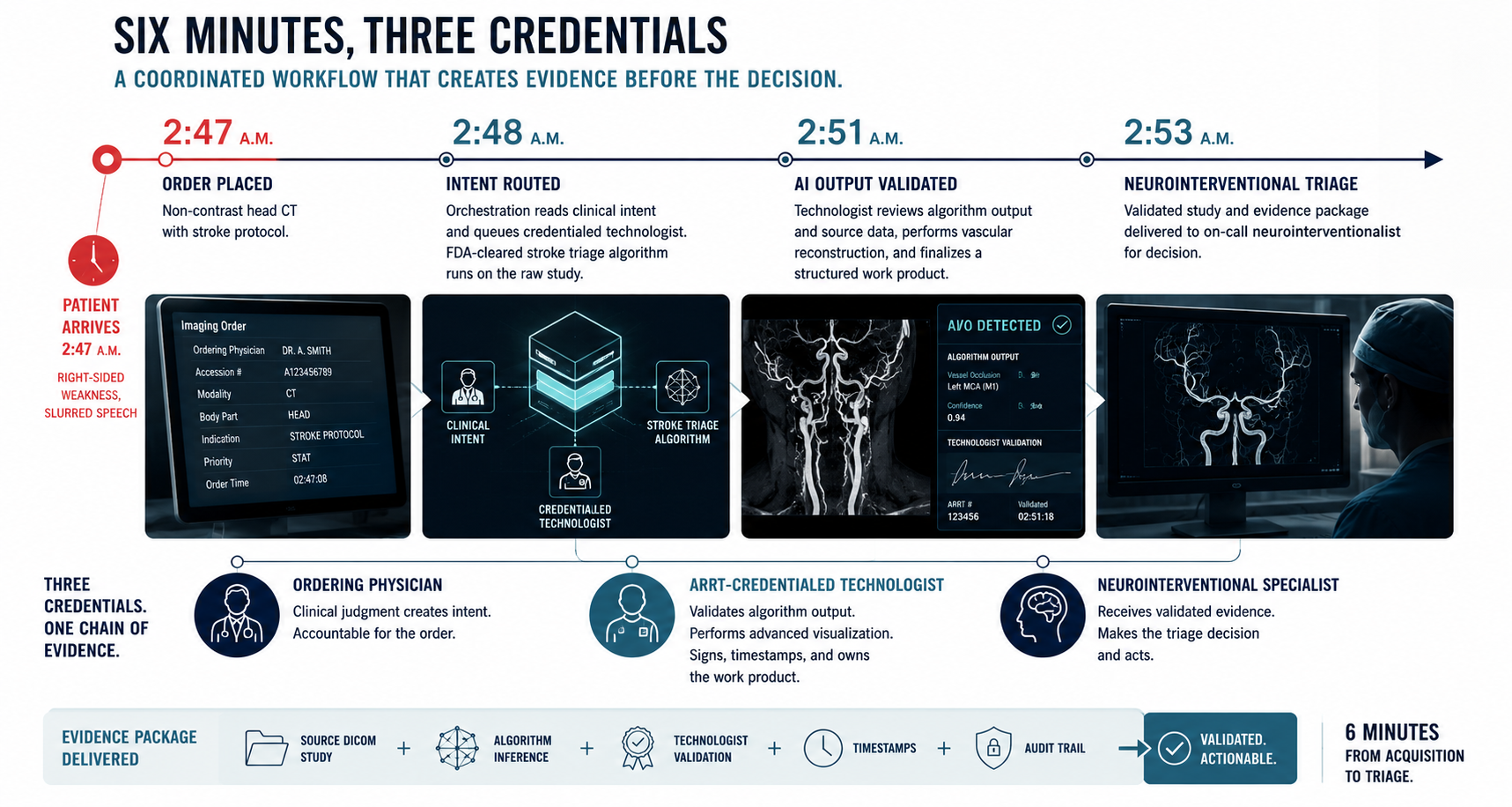
A patient arrives at the ED at 2:47 a.m. with right-sided weakness and slurred speech. The on-call physician orders a non-contrast head CT with stroke protocol. The order moves through the EHR carrying a structured payload: ordering physician identifier, accession number, modality, body part, indication, timestamp.
By 2:48 a.m., the orchestration layer has read the clinical intent off the order and queued an ARRT-credentialed radiologic technologist whose credential set includes Code Stroke Certification. The same orchestration layer fires the FDA-cleared stroke triage algorithm against the raw study.
By 2:51 a.m., the technologist has the algorithm output and the source DICOM data side by side. She validates the large vessel occlusion flag, performs the vascular reconstruction the radiologist will need for thrombectomy planning, and finalizes a structured work product that carries her credential number, her validation timestamp, and the algorithm vendor's signed inference.
By 2:53 a.m., the on-call neurointerventionalist has the validated study on screen. Six minutes from study acquisition to neurointerventional triage. Three credentialed parties have produced documented evidence. None of them could have produced any of it without the others.
In a hospital running the previous architecture, the same handoff took twenty-five minutes. The work product was less structured. The credential chain was thinner.
The orchestration platform is called Strings. The technologist tier is called 3DR Labs. Twenty-one years old. Headquartered in Louisville, Kentucky. Three hundred ARRT-credentialed technologists across the country. Sixty-five FDA-cleared AI algorithms in the clinically integrated platform that augments their work. It charges per click. No subscription. No minimums.
Per click. That is the entire pricing page.
Robert Falk founded the company in 2005. He is a practicing neuroradiologist. AI did not yet exist as a clinical product. The architectural choice he made was to pull a specific stage of the radiology workflow out of the radiologist's hands and turn it into an independent, credentialed, third-party tier. That choice is the reason the rest of this newsletter is worth writing.
Tuesday's argument, in one paragraph
On Tuesday I wrote about the Pivot Shift test. A physical-exam maneuver for ligament integrity, documented as performed on patients the clinician had never met. Generated by a software platform. Routed through a telemedicine front. Paid by Medicare. More than a billion dollars billed, more than $450 million paid. [9]
The Brett Blackman conviction landed Wednesday, May 14. The day before, CMS imposed a nationwide six-month enrollment moratorium on new hospice and home health agencies citing systemic fraud in workflows built to extract from vulnerable patients. The agency had already imposed a similar moratorium on DME suppliers earlier in 2026. [1] The same Wednesday, the New York Times ran Geoffrey Hinton publicly retracting his 2016 prediction that AI would replace radiologists. [2]
Three federal moments. Twenty-four hours. One architectural question underneath all of them. The workflow that can be designed for extraction can also be designed for delivery. The proof case is the 2:47 a.m. scene this newsletter opened with. Whoever holds the credential decides whether a claim can be generated.
The numbers
Imaging has been quietly winning the federal AI clearance race for half a decade. The FDA's AI and machine learning enabled medical device list, updated March 2026, shows 1,451 cumulative authorizations through end of 2025. Radiology accounts for 1,104 of them. Seventy-six percent. [3] Every other medical specialty in the United States combined accounts for the remaining twenty-four.
Of the 28 devices cleared with a Predetermined Change Control Plan in 2024, the federal scaffolding for governing in-market AI model updates, 15 were radiology. [4] The FDA finalized the PCCP guidance on December 4, 2024. [5] Radiology piloted the discipline.
The AI works because the workflow underneath it was built right first. Every imaging study generated in an American hospital carries structured metadata before it reaches a radiologist. Ordering clinician. Accession number. Modality. Body part. Device serial number. Technologist ID. Timestamps to the second. PACS systems log every query, retrieval, view, export, and modification against the IHE Audit Trail and Node Authentication profile. The audit trail came before the AI. The credentialed validator came before the cleared device. The accession number came before the inference. None of that was designed for AI. All of it is the reason the AI works.
What 3DR Labs actually built
Most readers of this newsletter know what teleradiology is. A board-certified radiologist somewhere else reads your hospital's study and signs the report. NightHawk did it overnight. vRad does it at scale. Subspecialty groups do it for second opinions. The market is roughly $7.6 billion in 2026. [22]
3DR is not that. 3DR has no radiologists on staff.
What 3DR does is the stage of the radiology workflow that sits between the scanner and the reading radiologist. The advanced visualization work. CT angiograms reconstructed into vascular trees the surgeon can plan from. Bone removed from contrast studies. Cardiac function quantified from raw four-dimensional data. Tumor volumes measured. Calcium scored. Aortic dilations measured. Liver iron quantified. Pre-surgical orthopedic reconstruction. Code stroke triage processing.
That work used to be the reading radiologist's job. The radiologist would receive raw data from the scanner, sit at a 3D workstation, manipulate the images themselves, and then dictate a report. The quality of the post-processing depended on the radiologist's skill with the workstation, their time pressure that shift, and which software the institution had bought. Variability was the norm. The advanced visualization layer was not its own thing. It was a thing radiologists did between getting the scan and writing the report.
Falk pulled it out of the radiologist's workflow in 2005. He made it an independent credentialed tier. [23] An ARRT-credentialed technologist, trained specifically in advanced 3D post-processing, sat in the middle of the workflow. The technologist's work product was the input the reading radiologist depended on. The technologist's credential, validation timestamp, and quality metrics travelled with the case.
What that did was unbundle two parts of the workflow that had always been one. The act of generating diagnostic evidence (the 3D reconstruction) became separable from the act of interpreting diagnostic evidence (the read). Two credentialed parties were now required where there had been one. The radiologist could not produce the read without the technologist's work product. The technologist could not bill without the radiologist's read.
That separation, in 2005, anticipated something nobody was talking about yet. It anticipated AI safety architecture.
When FDA-cleared AI tools began arriving at scale after 2018, they slotted into the workflow at the technologist tier. The technologist now uses sixty-five FDA-cleared algorithms in 3DR's AI Labs, a clinically integrated AI platform, as part of their post-processing work. [12] The AI does not produce a result that goes directly to the radiologist. The credentialed technologist validates the AI output, integrates it into the post-processed study, and signs the work product. The validation runs on a desktop workstation or a mobile device, which means the credentialed review is not tied to a single physical reading room. The AI is an augmentation tool. Not an autonomous reader.
That separation is not what algorithm-orchestration platforms like EnvoyAI, Sectra Amplifier, deepc, Harrison.ai's Open Platform, or RapidAI's marketplaces do. Those platforms route AI inputs and outputs between hospital PACS systems and algorithm vendors. They do not put a credentialed clinical worker in the validation chain. They are infrastructure. 3DR is a credentialed service tier with a clinically integrated AI platform as a component of how its credentialed workers do their job.
The choice was made at the workflow layer before the first transaction.
Strings: pre-interpretation evidence versus post-hoc documentation
In September 2025, 3DR acquired Strings. [19] On March 10, 2026, Strings shipped what the company describes as the first intent-driven agentic AI in radiology operations. The product reads clinical intent off the EHR order, routes the study to the correct AI tool and the correct technologist queue, and orchestrates the handoffs between PACS, the algorithm vendor, the technologist, and the report destination without a human pulling levers. [20]
What "intent-driven" means at the engineering level is the same primitive that DMERx ran in reverse.
DMERx, the platform at the center of Tuesday's HealthSplash conviction, took five fields and industrialized them. A doctor's name. A National Provider Identifier. A CPT or HCPCS code. A signature. A free-text indication. No accession number. No device serial. No technologist ID. No audit log. No credentialed second party. The Pivot Shift test and the One-Legged Stand test appeared in DMERx templates by the thousands because nothing in the workflow ever generated evidence that a physical exam had actually been performed. [9]
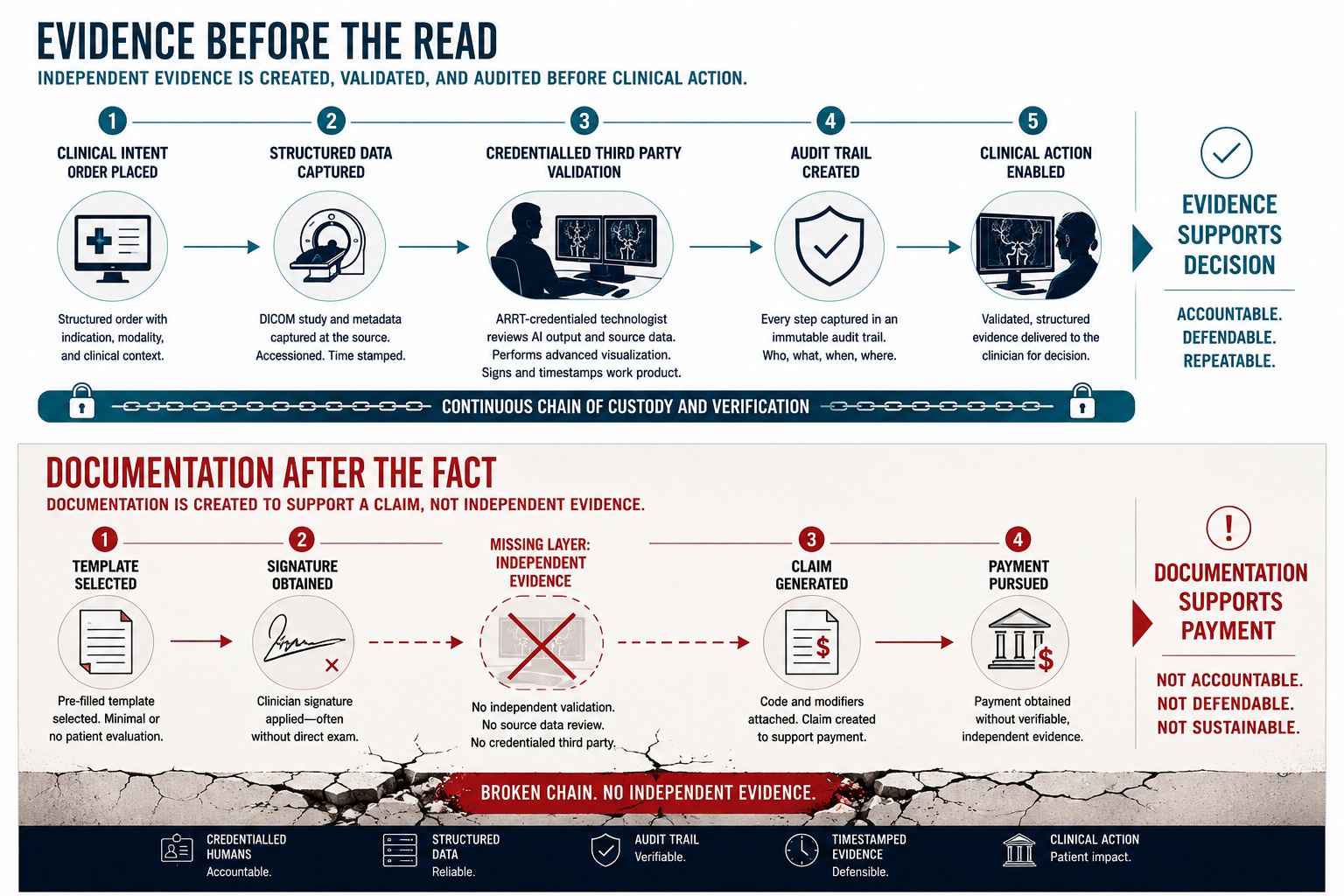
DMERx generated documentation after the encounter to make a fake encounter look real. 3DR and Strings generate evidence before the read to make the real encounter possible. Same primitive. Opposite product.
The clinical surface area where the 3DR primitive matters most is stroke. The Brainomix 360 platform on which the underlying triage runs was the subject of the largest real-world stroke AI evaluation ever published, in Lancet Digital Health in December 2025. Across 452,952 patients at all 107 NHS hospitals in England, endovascular thrombectomy rates doubled from 2.3 to 4.6 percent after Brainomix 360 Stroke implementation. [21] Doubled. At national scale.
Strings reports the platform saves more than 467 clinician-effort hours per month per site. Nineteen minutes of orchestration time, removed from the front end of every stroke workflow that uses it, is a clinical lever, not a productivity slide.
The pattern OpenAI shipped in October 2025
In November 2024, Anthropic published the Model Context Protocol as an open standard for connecting AI applications to external tools and data. The protocol defines a host application, a standardized way for tools to advertise their capabilities through JSON Schema, structured contracts for tool calls, OAuth 2.1 credentialing for tool authentication, and an audit trail by default. OpenAI adopted MCP in March 2025. In October 2025, OpenAI announced the Apps SDK, which extends MCP with an interactive interface layer, and in December 2025, Anthropic, Block, and OpenAI co-established the Agentic AI Foundation under the Linux Foundation and donated MCP as industry infrastructure. [37] By March 2026, the protocol had surpassed 97 million monthly SDK downloads. [38] Pilot apps inside ChatGPT include Booking.com, Canva, Coursera, Figma, Expedia, Spotify, and Zillow. [39]
The architecture is straightforward. A host application reads user intent off the conversation. The model decides which credentialed tool to invoke from a curated marketplace. The tool returns structured output through a standardized protocol. Every interaction is logged. App review gates what enters the marketplace.
That is the architecture radiology has been running on since the late 1990s, in modality-specific form. The host (PACS). The standardized protocol (DICOM). The audit trail (IHE ATNA). The credentialed tool marketplace (FDA-cleared algorithms with PCCP for in-market updates). Order intent routes to the tool. Structured output returns. Every interaction is logged.
What 3DR added in 2005 is the part of the architecture the AI industry has not yet figured out: a credentialed third-party human worker tier between the model output and the final consumer of the output. Strings is the orchestration layer. AI Labs, the clinically integrated platform, is where the 65 FDA-cleared algorithms become tools the technologist actually uses. The 300 ARRT-credentialed technologists are the validation tier the consumer-AI version of this pattern does not include.
What OpenAI standardized in October 2025, radiology operationalized in 2005, with a credentialed-worker tier on top. The federal question is which other care modalities adopt the same pattern next, and which keep operating on the trust-the-signature model long enough to be the next enforcement moratorium.
Where the architecture is missing
The CMS moratorium that took effect May 13 covers hospice and home health enrollment. The DME moratorium took effect earlier in 2026. The DOJ conviction landed Wednesday. The fraud pattern is the same across all three modalities. The architectural gap is also the same.
In hospice, Medicare eligibility requires a physician certification that the patient has six months or fewer to live. One certifying physician. One signature. No credentialed third-party prognosis review independent of the certifying physician. The OIG has documented hospice billing for patients with multi-year actual survival. The certifying physician knew, or did not bother to know, that the prognosis criterion was not met. The workflow generated documentation. It did not generate independent evidence.
In home health, Medicare requires a face-to-face encounter and physician certification of medical necessity. The certifying physician documents the encounter and signs the order. No credentialed third-party encounter verification. The OIG has documented home health agencies billing for services where the supervising physician had no recent visit with the beneficiary. Again, documentation. Not independent evidence.
In DME, Medicare requires a written order with documented medical necessity. One physician signature. No credentialed evaluator independent of the DME supplier verifying that the indication is supported by an exam. DMERx industrialized the gap. A signed order with a free-text indication is the entire evidentiary bar.
Telemedicine consult fraud rides the same gap. The encounter happens. The platform generates a note. The note flows into a claim. There is no credentialed pre-encounter work product that constrains what the note can claim to contain.
The pattern is the same. A single billing party generates the documentation that supports their own claim. There is no credentialed third-party tier producing structured evidence that the billing party depends on. The workflow has one credential in the chain, and that credential belongs to the party that gets paid.
3DR is the radiology version of what those modalities need at architectural specification. Two credentials in the chain. Structured work product from the upstream credentialed tier. The downstream billing party cannot generate a claim without the upstream evidence. The upstream evidence cannot be fabricated because it carries the upstream credential and timestamp. Each tier audits the other.
That architecture is what twenty-one years of radiology workflow design built. The other modalities are still operating on the trust-the-signature model. The federal enforcement spend responding to that gap is now measured in billions per year.
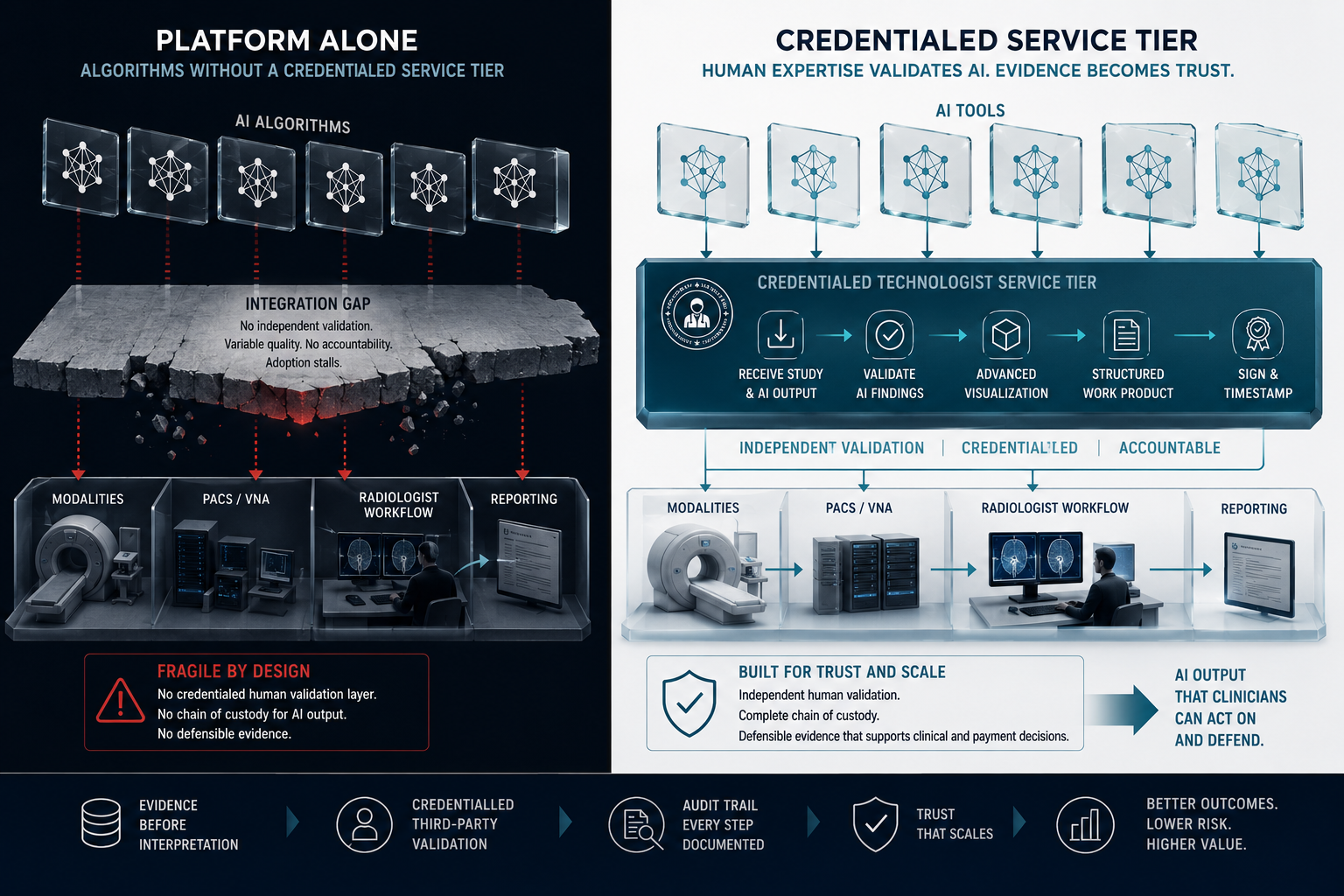
The platform without services is fragile
The same architectural choice has been tested in radiology itself, and the test broke the other way.
On September 8, 2025, Bayer announced it was discontinuing Calantic Digital Solutions and deprioritizing Blackford Analysis, its entire radiology AI platform business, citing slow clinical adoption and misaligned business models. [21A] Blackford carried more than 150 third-party AI applications at the time. Signify Research analyst Umar Ahmed told AuntMinnie the move took nearly 10 percent of the radiology AI platform spend off the board overnight.
Bayer ran a platform. Hospitals subscribed. Algorithms aggregated. The credentialed validation tier was the hospital's own radiologist, who was supposed to evaluate AI output between cases. The clinical adoption never caught up to the technical capability. The platform shut down.
3DR runs a service. Hospitals pay per click. Algorithms come and go from the platform. The credentialed technologist in the loop is the constant, and the credentialed technologist is the architectural primitive the platform alone cannot reproduce.
Three hundred ARRT-credentialed technologists are the moat the platform layer alone cannot build.
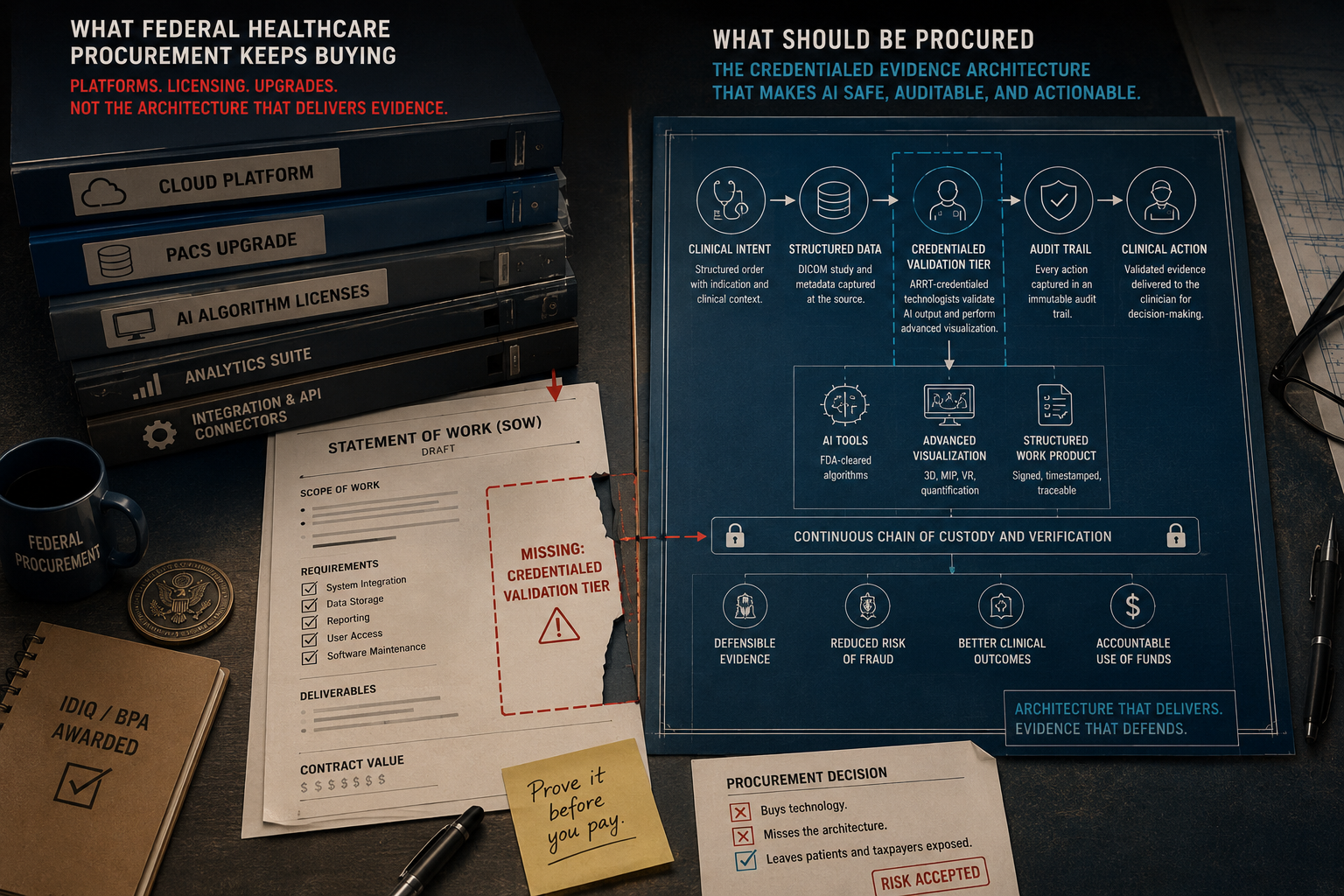
What federal radiology procurement just failed to buy
The federal procurement record on radiology AI is a study in contrast.
DHA buys directly when it sets out to. The agency serves 9.6 million active-duty, retiree, and family beneficiaries. On November 4, 2024, it awarded Volpara Health a five-year $7.3 million contract to deploy Volpara Patient Hub mammography reporting across the Military Health System. [28] Previous generations of Volpara's software have been in DoD service since 1990. Modest dollars. Decades-deep incumbency. A working pattern.
The VA's National Teleradiology Program tells the inverse story. NTP serves 125 unique VHA sites across all 18 Veterans Integrated Service Networks and interprets roughly 1.5 million exams a year. The PACS refresh was awarded in September 2023 to Frontier Acquisitions LLC of San Antonio as prime, with Mach7 Technologies as the Vendor Neutral Archive, Blackford as the AI platform layer, Nuance for voice recognition, and Microsoft Azure for cloud hosting. [29] Phase I had a contract value of A$11.7 million. Phase II ran to A$47.9 million. The architecture was modern, vendor-neutral, and on paper looked like what right looks like.
The deployment did not survive contact with the procurement environment.
On January 31, 2026, Mach7 CFO Daniel Lee told investors on the company's Q2 FY26 earnings call that the company's Contracted Annual Recurring Revenue had declined A$2.9 million quarter over quarter. He said the decline was driven primarily by the removal of the NTP project from the CAR backlog. [30] The deployment did not complete. Blackford, the AI platform layer the cancelled NTP architecture was built around, had been deprioritized by Bayer four months earlier. The federal procurement vehicle was tied to a platform architecture that did not include a credentialed service tier, while the platform vendor was itself collapsing.
On May 1 I wrote about the VA Strategic Acquisition Center certifying a single source to upgrade NTP PACS infrastructure three months after five qualified sources were already delivering on a competing architecture. The Mach7-Frontier-Blackford removal from CAR backlog is the documented resolution of that fight. The original award did not deliver.
On March 19, 2026, VA Technology Acquisition Center in New Jersey posted Solicitation 36C10B26Q0213. A sole-source synopsis solicitation to Intelerad Medical Systems for an in-place upgrade of the existing 2013-era IntelePACS from version 4.9 to 5.7, hosted in VAEC. Response deadline March 20, 2026. One day. Statutory authority: FAR 6.103-1, Only One Responsible Source. Contracting Officer: Kathryn Pantages, the same CO who managed the original 2022 RFI that became the cancelled 2023 architecture. [29A] The cancelled September 2023 Frontier-Mach7-Blackford modernization has been functionally abandoned. The 2013 Intelerad system has been extended through at least 2027. Second consecutive single-source determination on the same program, same CO, same legacy vendor.
Federal procurement has not built the vehicle that buys the architectural primitive. The Volpara contract proves the pattern is structurally possible. The NTP cancellation proves what happens when the federal vehicle buys the platform layer without the services layer underneath it.
The people downstream
The MTF radiologist reading at the top of her capacity, whose pre-validated worklist multiplies her output without multiplying her caseload, because the credentialed technologist tier has already done the advanced visualization the read depends on.
The DOJ National Fraud Enforcement Division auditor who sees, in an imaging audit trail, two credentialed parties and a structured work product where in a DME audit trail she sees one signature and a templated indication, and recognizes in that asymmetry why one workflow was prosecutable and the other was not.
The Navy corpsman in a Pacific theater waiting on a teleradiology read whose stroke study could move through the same six-minute three-credential window the 2:47 a.m. scene described, or could move through whatever PACS architecture the VA Strategic Acquisition Center eventually contracts for, depending on whether the federal procurement vehicle catches up to the architectural primitive that already exists.
You cannot recruit your way out of the radiology workforce gap. The Neiman Health Policy Institute projects supply growth of 25.7 percent through 2055 while demand grows comparably. The shortage persists for three decades without intervention. Imaging interpretation turnaround time more than doubled between 2014 and 2023, with CT up 318 percent and MR up 256 percent. [36]
Mayo Clinic's radiology department has grown 55 percent to 400 radiologists since 2016 and runs more than 250 AI models, concentrated in radiology. The model works. The architecture exists. Mayo built one. What is missing is the federal procurement vehicle to buy it at scale, and the legislative imagination to require the credentialed-third-party architecture in the modalities CMS is currently shutting down to stop the fraud.
The corpsman in the Pacific is still waiting on a read.
The procurement language is still a Statement of Work draft away.
The foundation model layer underneath this whole architecture is its own story. That is the next one I will tell.
Let's roll.
Mary
Mission Meets Tech.
The views expressed in this newsletter are my own and do not represent the official position of any organization. This content is for informational purposes only.
MMT Premium
Want the capture intelligence behind this analysis?
MMT Premium subscribers receive the companion Capture Corner with this issue: the federal radiology AI procurement playbook with the Volpara/Patient Hub contract structure decoded, the documented NTP NextGen PACS cancellation paper trail mapped to the next acquisition window, the HCDS imaging-interface scope watchlist, the FDA PCCP guidance translated into federal procurement language ready to drop into a Statement of Work, the credentialed-third-party architectural specification translated into procurement requirements for non-radiology modalities (DME, hospice, home health, telehealth), and the named DHA and VA decision points where vendor-neutral orchestration architectures fit.
Founding Member rate: $199/year (locked permanently for the first 100 subscribers)
Standard rate: $249/year or $29/month
Plus: 48-hour early access, deep-dive solicitation analysis when major RFPs drop, direct Q&A access, and tool discounts.
Subscribe at missionmeetstech.com/pricing
Sources
[1] CMS, "CMS Announces Aggressive Nationwide Crackdown on Fraud with Six-Month Hospice and Home Health Agency Enrollment Moratoria," May 13, 2026.
[2] Steve Lohr, "A.I. Was Supposed to Replace Radiologists. It Hasn't," New York Times, May 14, 2026.
[3] FDA, "Artificial Intelligence and Machine Learning (AI/ML)-Enabled Medical Devices," March 2026 update; The Imaging Wire analysis, March 11, 2026.
[4] "Machine Learning-Enabled Medical Devices Authorized by the US Food and Drug Administration in 2024," PubMed Central.
[5] FDA, "Marketing Submission Recommendations for a Predetermined Change Control Plan for AI-Enabled Device Software Functions," final guidance, December 4, 2024.
[9] U.S. Department of Justice, superseding indictment in United States v. Brett Blackman, Gary Cox, and Gregory Schreck, Southern District of Florida.
[12] 3DR Labs, "About 3DR Labs" and "AI Labs, vendor-agnostic clinically integrated AI platform."
[19] Arsenal Capital Partners, "3DR Labs Acquires Strings," September 23, 2025.
[20] National Law Review, "3DR Labs Redefines Imaging Operations with Strings First-of-Its-Kind Intent-Driven Agentic AI," March 2026.
[21] Lancet Digital Health, "Artificial intelligence imaging decision support for acute stroke treatment in England: a prospective observational study," December 2025; Brainomix press release.
[21A] AuntMinnie, "Bayer Pivots Away from AI Platform Business," September 8, 2025; The Imaging Wire, "Investment in AI Platform Company Blackford," September 7, 2025.
[22] Mordor Intelligence, "Teleradiology Market Size, Trend Analysis & Growth Report 2026."
[23] 3DR Labs, company founding history; HigherGov, "3DR Labs II, LLC, Federal Awardee Profile"; 3DR Labs, "Appointment: Michael Jackman, CEO," November 4, 2024.
[28] Volpara Health, "Volpara Secures U.S. Defense Health Agency Contract to Modernize Mammography Services," November 4, 2024.
[29] PR Newswire, "Mach7 Technologies Selected as a Solution Provider for VHA National Teleradiology Program NextGen PACS," September 6, 2023.
[29A] SAM.gov, National Teleradiology Program PACS Upgrade, Synopsis Solicitation 36C10B26Q0213, posted March 19, 2026; sole-source to Intelerad Medical Systems under FAR 6.103-1.
[30] Defense World, "Mach7 Technologies Q2 Earnings Call Highlights," January 31, 2026.
[36] Neiman Health Policy Institute, "New Studies Shed Light on the Future Radiologist Workforce Shortage," February 12, 2025; Christensen and Parikh, JACR; Neiman HPI, "Imaging Interpretation Turnaround Time More Than Doubled Between 2014 and 2023."
[37] Anthropic, "Introducing the Model Context Protocol," November 2024; Wikipedia, "Model Context Protocol," accessed May 2026; Linux Foundation, Agentic AI Foundation announcement, December 2025.
[38] DEV Community / industry tracking, "Complete Guide to MCP in 2026: Architecture, Implementation, and Enterprise Roadmap," April 2026.
[39] OpenAI, "Introducing apps in ChatGPT and the new Apps SDK," October 2025; The New Stack, "Inside OpenAI's Apps SDK," October 2025; OpenAI Developers, "MCP, Apps SDK," 2025.