DHA Is Replacing How It Buys. The Budget Already Voted.
A new acquisition model, a requirements process built to kill "bring me a rock," and a set of live contracts that show both already in motion.
Friends,
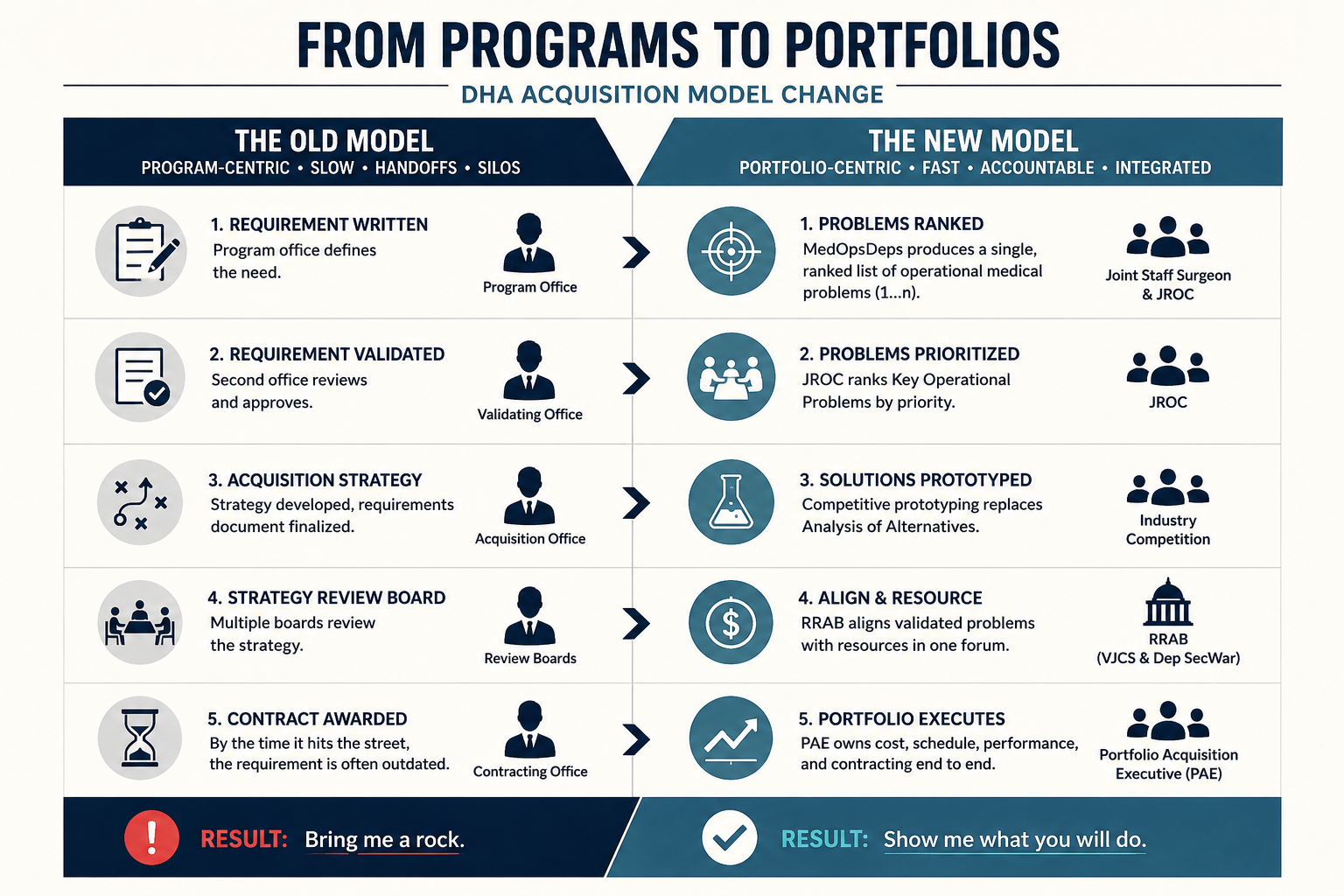
For thirty years the Defense Health Agency bought medical capability the same way the rest of the Department did. A program office wrote a requirement. A second office validated it. A third built an acquisition strategy around it. A board reviewed the strategy. By the time a contract hit the street, the requirement that started the process was often older than the technology meant to satisfy it. Industry has a name for the result. You bring the government a rock, and they tell you they wanted a different rock, and the cycle starts over.
That model is being replaced. All of it. On April 20, 2026, DHA stood up a new acquisition structure. In July 2026 it reaches Full Operating Capability. The change is large, it is statutory, and the FY2027 budget request already tells you where it is pointed.
This issue covers four things. What the new structure is. Who runs it. How it maps to the budget. And whether the requirements reform underneath it actually fixes the rock problem, or just moves the rock.
What changed
The unit of acquisition is no longer the program. It is the portfolio.
Section 1802 of the FY26 NDAA, signed December 18, 2025, created 10 USC 1732 and ordered every Department of War component to convert its Program Executive Offices into Portfolio Acquisition Executives by December 2027. A PAE owns a whole portfolio end to end. Cost, schedule, performance, the contracting officer inside the team, milestone decision authority pushed down to the lowest sensible level. One accountable official instead of a relay race of offices.
DHA built three portfolios. Medical Products owns devices, drugs, blood, diagnostics, simulation, the materiel that goes forward with the force. That is the warfighting kit. Medical Services owns the clinical service lines, managed care, professional services, readiness support. A third portfolio for digital and software arrives at FOC, named Medical Digital Solutions in the May 12 acquisition synch deck, though the org chart still carries the legacy label "Medical Software and Business Systems." If you sell software or virtual care, your portfolio owner is not fixed until the July charter publishes.
Underneath the structure sits a new way of validating what gets bought. The old Joint Capabilities Integration and Development System is gone, disestablished by a Secretary of War memo on November 7, 2025. In its place, for operational medicine, sits a process run out of the Joint Staff Surgeon's office called MedOpsDeps. It does something the old system never forced: it produces a single ranked list, one through n, of operational medical requirements, scored against a published rubric, before the money conversation starts. The Analysis of Alternatives is replaced by competitive prototyping. Build the thing, run it against a real operational scenario, show the outcome.
The validation machinery above it moved too. The Joint Requirements Oversight Council, the body that used to approve requirement documents, now ranks Key Operational Problems instead. It states the problem and its priority and leaves the solution open. A new Requirements and Resourcing Alignment Board, co-chaired by the Vice Chairman of the Joint Chiefs and the Deputy Secretary of War, becomes the single forum where the validated problems meet the money. For thirty years requirements and resourcing ran on separate tracks that rarely touched. The RRAB is the table built to make them touch.
The two memos that authorized this moved on the same day. Requirements reform and acquisition reform, November 7, together. For decades the two halves were reformed separately and never met. This time they were redesigned to fit.
Who runs it
Authority routes to specific offices now, and a vendor who knocks on the wrong door loses a quarter.
VADM Darin Via directs the Defense Health Agency, and the acquisition authority inside it runs to the Component Acquisition Executive, RDML Ivonne Arena, at the top of the DHA acquisition chain. Below that, three portfolio executives own the buying: one for Medical Products, the materiel that goes forward with the force; one for Medical Services, the clinical service lines and readiness support; and one for digital and software, the portfolio still being chartered. A separate research and development directorate sits alongside them. The Capability Trade Council, which replaces the old configuration steering board, now holds the authority to waive non-statutory technical standards, which means a requirement you have spent three years trying to meet may be one the Council decides not to enforce. The named owner of each portfolio, and which seats are still acting, is the kind of map a capture team needs in front of it; that roster lives in this week's Capture Corner.
One organization sits outside all of it. PEO DHMS, which runs MHS GENESIS, JOMIS, and the federal electronic health record work with VA, did not fold into a portfolio. Per the FY2027 budget documents it keeps its own executive authority and reports directly to the Under Secretary of Defense for Acquisition and Sustainment. The largest IT enterprise in military medicine is governed by different rules than everything around it. Hold that fact. It returns when the contracts come up.
The newest power center sits outside the PAE structure entirely. The Office of Warfighter Health Advantage consolidated five separate offices, the Director's Innovation Group, the Chief Data and Analytics Office, the Business Integration Division, the Digital Health Integration Office, and the Strategic Integration Group, into one shop reporting to the DHA Deputy Director. It controls the FY2027 IMIT growth line, and that line is where the budget starts to talk.
What the budget says
A reorganization is a theory until the money agrees with it. The FY2027 request agrees, and it does so in lines anyone can pull from the budget exhibits.
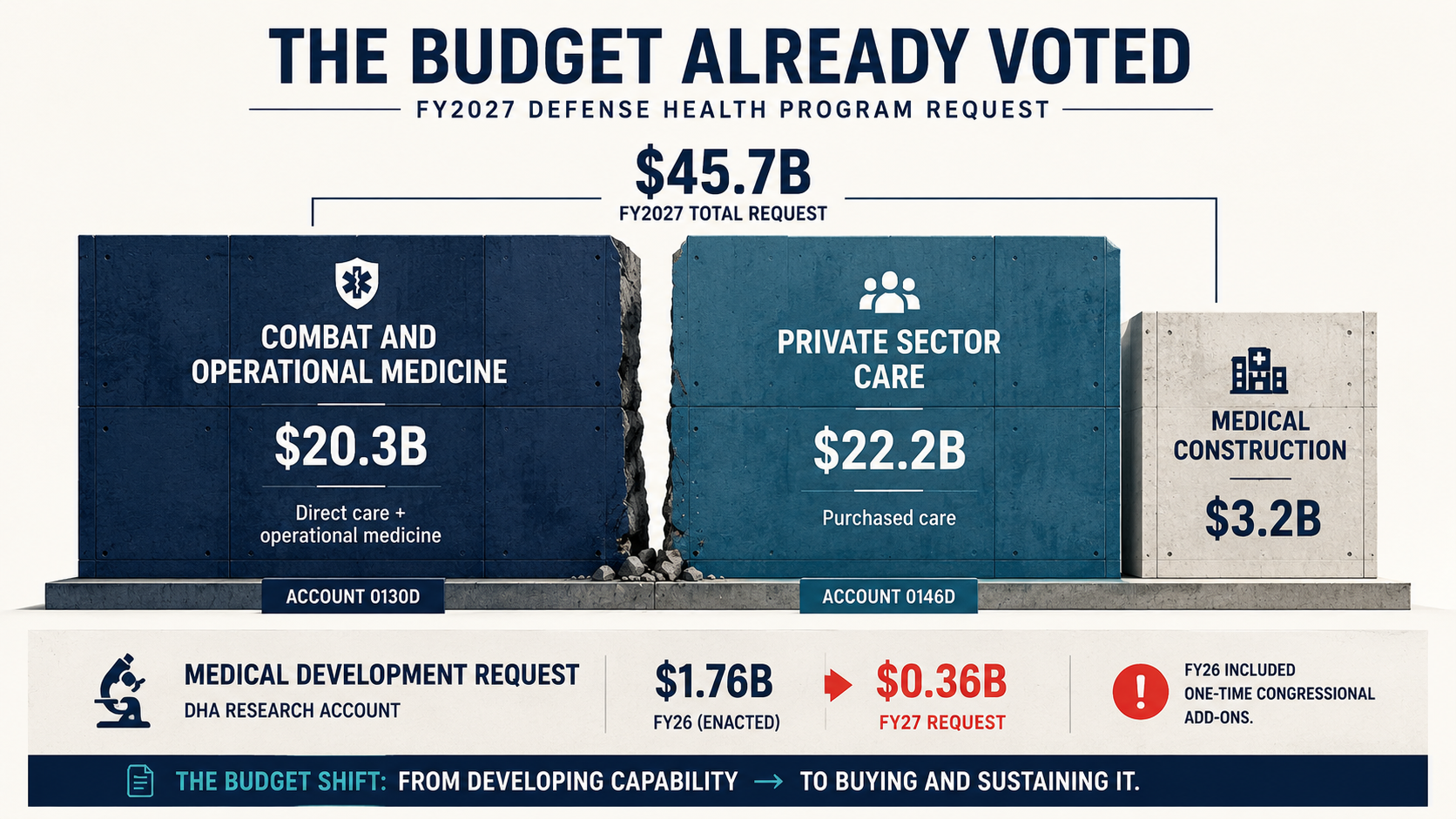
Start with the account structure, because it changed at the foundation. For decades the Defense Health Program funded everything from one account: the military treatment facilities, the in-house clinical workforce, and the purchased care that flows to civilian networks through TRICARE, all in the same pot. The FY2027 request splits that pot in two. Direct care and operational medicine become a new account, the Combat and Operational Medicine Program, at $20.3 billion. Purchased care becomes its own account, the Private Sector Care Program, at $22.2 billion. The exhibits carry them as accounts 0130D and 0146D. Add $3.2 billion in medical construction and the FY2027 request totals $45.7 billion, a 5% increase over FY26. One account now carries military medicine alongside the rest of the warfighting portfolio. The other carries the TRICARE bill.
The stated reason for the split is blunt: to keep rising TRICARE costs from hollowing out the military treatment facility system. Walling the two accounts apart means purchased-care growth can no longer quietly eat the money that staffs and runs the MTFs. Read what that does to the money you sell into. Purchased care, which years ago sat as a sub-line buried inside the old program, now has its own appropriation, its own account number, and its own visibility. It ran $20.20 billion in FY25 and $20.77 billion in FY26 when it was buried. At $22.2 billion in its own account it is the largest single growing target in the request, and for the first time it is severable and cuttable as one line. You do not give something its own account unless you intend to manage it as its own decision.
Now the line every R&D vendor reads first. Medical Development, the DHA research account that funds advanced development of medical products, shows $1.03 billion in FY25, $1.76 billion in FY26, and $0.36 billion in the FY2027 request. Before that reads as a collapse, know what is inside it. Most of the FY26 figure was one-time congressional add-ons, the medical-research plus-ups Congress appends above the request every year and almost always restores. The request strips them out. Congress will likely put much of them back, so the enacted number lands higher than the request. DoD Medical Information Exchange and Interoperability sits flat at $10 million. The procurement line for DoD Healthcare Management System Modernization, the GENESIS build money, is zeroed.
Read them together with that caveat in place. The honest signal is narrower. The base request funds readiness research below what Congress enacted last year, at the same moment the new requirements process ranks blood management, trauma and critical care, and medical data systems as its top demand categories. Stated priority and funded priority are not aligned, and the gap is the request betting Congress will close it. The build phase is ending. No successor build line sits behind it. The money is moving from developing capability to buying and sustaining it, exactly the shift a portfolio-and-prototyping model is designed to execute. The budget is the reorganization, expressed in dollars.
One more line, because it changes how you read the near term. Base Operations and Communications, now inside the Combat and Operational Medicine account, shows $2.46 billion in FY27 discretionary money, propped up by an additional $3.14 billion in one-time reconciliation funds drawn from PL 119-21. More than half of that account in FY27 is non-recurring. One-time money buys near-term services and sustainment, not durable program starts. It tells you where the fast, expiring dollars sit, and it tells you they expire.
How it shows up in live contracts
None of this is forecast. It is already in solicitations on the street.
The clearest example is the $300 million Defense Healthcare Management Systems Deployment Solutions IDIQ, proposals due April 21, 2026 after a final extension. DHA wrote it to behave like the new model rather than the old one. The agency will not evaluate price, and intends to select every qualifying offeror onto the vehicle. The first evaluation factor is a challenge scenario. Bidders had to propose a deployment plan for a named situation: one accredited overseas medical center with 250 beds, two community hospitals, five clinics, roughly 5,000 users and 50,000 beneficiaries across multiple time zones. That is competitive prototyping logic written into a procurement. Show me what you would do against this real problem, not how well you can mirror my requirements document. That is the answer to "bring me a rock," operating in a live RFP.
The richest example for understanding the limits is the recompete for MHS GENESIS itself, the Health Care Delivery Solutions follow-on. DHA ran a draft contract strategy RFI in December 2025 that asked industry to react to the acquisition approach before the requirement was final, with the stated goals of keeping pace with commercial technology and shortening the time to compete the follow-on. The new behavior is visible in how the buy is being shaped. The timeline tells the harder truth. Open competition cannot release until the system finishes its cloud migration, which puts a competed award no earlier than 2028. Until then the incumbent, Leidos, holds the work on a sole-source bridge of $1.131 billion, with a separate transition increment of $263.3 million. Confirm both against USASpending before relying on them. There is a wrinkle in the reporting line that cuts the other way. Because PEO DHMS answers to USD(A&S), the eventual competition does not need DHA acquisition-executive sign-off to move. The chain runs from PEO DHMS straight to the Under Secretary, not through the new portfolio structure at all. So the largest health IT program in the Department is being dressed in the new vocabulary, runs its actual dollars through a sole-source bridge to the incumbent, and sits on a faster approval lane than the portfolios that are supposed to be the fast ones. For a vendor that is opportunity and ambiguity in the same program.
The strategy itself shows how far the thinking has moved. The posted follow-on approach drops the prime systems integrator that every large federal electronic health record buy has leaned on, and keeps integration authority inside the government, with contractors supporting rather than steering. A 2024 GAO review found military clinicians rated GENESIS below the system it replaced, with about 39% agreeing it supported patient-centered care against 56% for the legacy system, and the dental module Dentrix flagged as a persistent failure. You do not rebuild the buying model for a system the people using it are happy with.
Two more vehicles show the budget shift landing on real money. The OMNIBUS IV small business on-ramp, the $10 billion medical R&D vehicle, had its solicitation pushed to late May 2026 explicitly to comply with the new FAR Overhaul guidance, which is the reform touching a live award timeline directly. And MQS2-NG, the clinical staffing recompete with a ceiling reported above $40 billion, uses a self-scoring technical worksheet rather than a written technical narrative, the same scenario-and-score logic the rest of the system is moving toward.
These are the vehicles in daylight. The full picture, every live PEO DHMS action sorted by what the reorg does to it, the production-authority gap that strands follow-on money before the July charters, and the lane structure for the GENESIS recompete now that there is no prime to team with, is mapped in this week's Capture Corner.
Does it fix "bring me a rock"
The rock problem has three layers, and the reform touches each one differently. Layer one shrinks the rock. Layer two closes the gap. Layer three is still stranded.
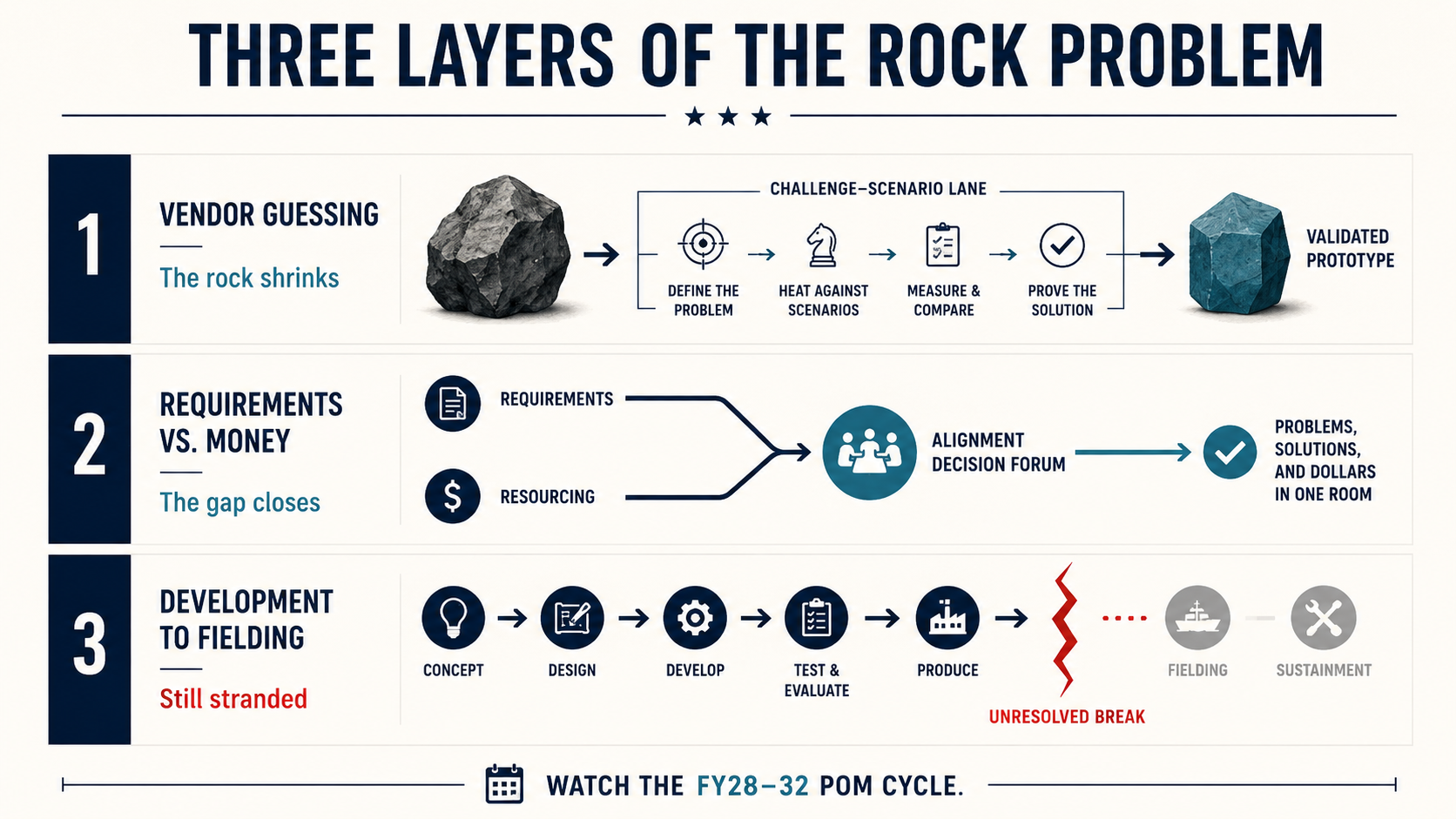
The first layer is the contractor guessing at what the government actually wants. This is the classic version, the one that gave the problem its name. Here the reform is working. Other Transaction authority, the Call for Solutions model, the Walter Reed and Kaiser Permanente prototype, and the $300 million deployment IDIQ all let a vendor build against a stated problem and demonstrate the result instead of decoding a specification and hoping. Show me what you would do is a better question than match my document. On this layer the rock is getting smaller.
The second layer is the gap between what gets validated and what gets funded. For thirty years a requirement could clear the old system and then sit, because requirements and money moved on separate tracks that rarely met. MedOpsDeps and the RRAB are built to close that gap. A single ranked list of operational medical problems now feeds the resourcing process directly, with one forum where the priority and the dollars get decided in the same room. This is the part that is genuinely new, and it is the part most likely to matter.
The third layer is the handoff from DHA development to a Service for procurement, fielding, and sustainment. This one is still broken, and the budget exhibits prove it. The traumatic brain injury blood assay cleared the FDA and reached full-rate production in May 2025. Its transition to sustainment is not projected until FY28, and the test cartridges carry a six-month shelf life, which turns a fielding delay into a supply problem. Field-portable ultrasound is not projected to transition until FY30. The capability exists now. The path to the warfighter runs years long, and the agreement that defines who owns the handoff is still unwritten.
So the mechanism is sound on two layers and absent on the third. The honest caution runs underneath all three. A ranking process is only as good as its inputs, and the MedOpsDeps rubric concentrates 40% of its weight in the Joint Medical Estimate, upstream, where a vendor can least see it and least influence it. A faster downstream process that starts from a poorly chosen problem just reaches the wrong rock faster. The reform may not eliminate the rock so much as move it, from the contracting shop to the requirements shop.
It is too early to call. The structure reaches Full Operating Capability in July 2026. The first full requirements cycle under the new rubric runs this summer. Then the test. Watch the FY28 to FY32 program objective memorandum cycle. That is where the theory meets the money, and that is where you learn whether the rock problem was solved, moved, or merely renamed.
Both sides of the procurement table
For the government program officer, the new model trades the safety of process for the exposure of speed. There are fewer offices to share the blame and one PAE who owns the outcome. Authority and accountability arrived in the same box.
For the contractor, the capture plan that worked in 2023 is now a liability. The work is to map every offering to a portfolio, to a budget line that is growing rather than shrinking, and to a scenario you can demonstrate against rather than a specification you can comply with. The R&D vendor whose business rode the Medical Development plus-ups needs a new plan, because the request does not carry them and congressional adds are never guaranteed. The vendor positioned on sustainment, deployment, and purchased-care support is reading a budget that is moving toward them.
The reason any of this matters sits at the far end of an evacuation chain. Disease and non-battle injury, not battlefield wounds, drive most of what pulls troops off the line, and the largest share of that is behavioral health and the ordinary medicine of keeping a force healthy. A surgeon who sees only routine garrison cases cannot hold trauma proficiency for the day it is needed. That is why DHA is buying complex case volume from civilian systems like the Walter Reed and Kaiser Permanente partnership, and why the budget walled purchased care into its own account. Most vendors build the pitch around the fraction that looks like war. The larger demand is everything else, and the new budget is moving toward it.
A separating aviator with a behavioral health diagnosis does not know which portfolio owns the program that might keep her flying. A clinician at a duty station does not care which account funds the record system she fights every shift. They need it to exist. To work in the field. To arrive before deployment. The whole apparatus, the portfolios, the rubric, the prototyping, the walled-off account, exists to make that last clause true. The next year decides whether it does.
Let's roll.
— Mary
Mission Meets Tech
The views expressed in this newsletter are my own and do not represent the official position of any organization. This content is for informational purposes only.
This week's Capture Corner is live for Founding Members
The premium companion turns this issue into a capture tool. It maps every live DHA medical contract vehicle by what the reorg does to each one, names the production-authority gap that strands follow-on OTA money until the July charters publish, reads the ranked FY28-32 requirements list as a buy list you can score your offering against, and lays out the DHA-to-Service transition gap as work you can win now. It closes with a 60-day sequence run against the real submission windows.
$199/year, first 100 seats still open. Founding Members get the Capture Corner with every Friday issue, plus the monthly MedOpsDeps and DHA contracting calendar and the quarterly PAE bench tracker. Lock the rate now; it does not return.
Sources
[1] Crowell & Moring LLP, "The FY 2026 National Defense Authorization Act," December 2025, https://www.crowell.com/en/insights/client-alerts/the-fy-2026-national-defense-authorization-act
[2] Greenberg Traurig LLP, "FY 2026 NDAA: The Substantial Impact of the Fiscal Year 2026 National Defense Authorization Act on Federal Procurement Law," February 2026, https://www.gtlaw.com/en/insights/2026/2/fy2026ndaa/fy-2026-ndaa-the-substantial-impact-of-the-fiscal-year-2026-national-defense-authorization-act-on-federal-procurement-law
[3] Secretary of War, "Transforming the Defense Acquisition System into the Warfighting Acquisition System," November 7, 2025, https://media.defense.gov/2025/Nov/10/2003819439/-1/-1/1/TRANSFORMING-THE-DEFENSE-ACQUISITION-SYSTEM-INTO-THE-WARFIGHTING-ACQUISITION-SYSTEM-TO-ACCELERATE-FIELDING-OF-URGENTLY-NEEDED-CAPABILITIES-TO-OUR-WARRIORS.PDF
[4] The White House, "Modernizing Defense Acquisitions and Spurring Innovation in the Defense Industrial Base," Executive Order 14265, April 9, 2025, https://www.whitehouse.gov/presidential-actions/2025/04/modernizing-defense-acquisitions-and-spurring-innovation-in-the-defense-industrial-base/
[5] Department of War, FY2027 Defense Health Program budget exhibits (O-1, R-1, P-1), Operation and Maintenance, RDT&E, and Procurement displays, accounts 0130D and 0146D, May 2026.
[6] Washington Technology, "DHA starts the bidding for $300M tech deployment support contract," April 8, 2026, https://www.washingtontechnology.com/contracts/2026/04/dha-starts-bidding-300-tech-deployment-support-contract/412707/
[7] Healthcare IT News, "DHA offers $300M for health IT deployment support," April 10, 2026, https://www.healthcareitnews.com/news/dha-offers-300m-health-it-deployment-support
[8] Defense Health Agency, Health Care Delivery Solutions (HCDS) Electronic Health Record Follow-on (MHS GENESIS), Notice ID HT003826X0000, RFI posted December 2025, RFI responses due August 30, 2026; competitive RFP not yet issued.
[9] OST Global Solutions, "DHA OMNIBUS IV On-Ramp: 8(a) Set-Aside Confirmed with Late May 2026 Solicitation Date," April 14, 2026, https://www.ostglobalsolutions.com/10b-dha-omnibus-iv-on-ramp-updated-8a-set-aside-confirmed-with-late-may-2026-solicitation-date/
[10] Col. (Dr.) Jeremy W. Cannon, USAFR (Ret.), Statement to the Senate Armed Services Committee, "Stabilizing the Military Health System to Prepare for Large-Scale Combat Operations," March 11, 2025, https://www.armed-services.senate.gov/imo/media/doc/statement_of_colonel_dr_jeremy_w_cannon_usafr_ret.pdf
[11] Defense Health Agency, "Walter Reed launches historic partnership with Kaiser Permanente to bolster military medical readiness," February 13, 2026, https://walterreed.tricare.mil/News-Gallery/Articles/Article/4408656/walter-reed-launches-historic-partnership-with-kaiser-permanente-to-bolster-mil
[12] Department of War, FY2027 Defense Health Program Budget Request Overview, Combat and Operational Medicine Program (0130D) and Private Sector Care Program (0146D) account restructuring and stated rationale, May 2026.
[13] U.S. Army Medical Research and Development Command, Medical R&D Acquisition Synch briefing, May 12, 2026 (MedOpsDeps scoring rubric; ATBI and field-portable ultrasound transition timelines).
[14] Department of War, Warfighting Acquisition System implementing guidance, December 4, 2025 (JROC reorientation to ranking Key Operational Problems; Requirements and Resourcing Alignment Board).
[15] U.S. Government Accountability Office, "Electronic Health Records: DOD Should Set Goals and Measure Progress to Improve MHS GENESIS User Experience," GAO-24-106187, April 2024.